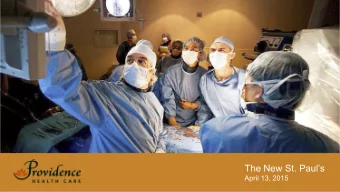
Federal Fiscal Year 2017-18 CHASE Fee Program June 21, 2018
Overview ➢ CHASE Overview ➢ Fee and Payments Methodologies ➢ Net Reimbursement Overview ➢ Payment to Cost Ratio ➢ Reconciliation Process Overview 2
Overview Program Goals Increase hospital reimbursement for Medicaid and uninsured • patients Fund hospital quality incentive payments • Expand health care coverage in Medicaid and Child Health • Plan Plus (CHP+) programs Reduce uncompensated care costs and the need to shift • uncompensated costs to other payers 3
Overview $370 million in net reimbursement 1 for hospitals between • October 2017 through September 2018 ➢ Net reimbursement reflects direct supplemental payments minus total CHASE fees and does not include revenue received by hospitals from coverage expansion $1.27 billion in total supplemental Medicaid & DSH payments, • including $97.6 million in quality incentive payments 4
Overview Provides health care coverage to more than 501,500 • Coloradans as of September 30, 2017: ➢ 376,000 adults without dependent children ➢ 93,000 Medicaid parents ➢ 25,000 CHP+ children and pregnant women ➢ 7,500 working adults and children with disabilities No General Fund expenditures • 5
Federal CHASE Fee Match from from CMS Hospitals Cash Fund (CHASE Fee + Federal Match) Increased Payment to Expanded Coverage to Hospitals Colorado Citizens 6
Overview Net Patient Revenue (NPR) – limiting total CHASE fees that • can be collected Upper Payment Limit (UPL) – limiting total supplemental • payments that can be paid Disproportionate Share Hospital (DSH) Limit – limiting • hospital specific DSH payments that can be paid 7
Overview Net Patient Revenue (NPR) CHASE Fee collection limited to 6% of actual NPR • Estimated using historical data inflated forward • Inpatient NPR = (Inpatient Revenue / Total Hospital Revenue) • * Total Hospital NPR * Inflation Outpatient NPR = (Total Hospital NPR – Inpatient NPR) * • Inflation 8
Overview Upper Payment Limit (UPL) Supplemental payment limited to UPL • Maximum Medicaid is allowed to reimburse to hospitals • Aggregate, not hospital-specific limit • Completed for both Inpatient and Outpatient services • UPL Room = Medicaid cost – Medicaid fee for service • payments – non-CHASE supplemental payments 9
Overview 10
Overview 11
Overview Disproportionate Share Hospital (DSH) Limit DSH supplemental payment limited to DSH limit • DSH limit = Medicaid plus uninsured cost minus Medicaid plus • uninsured payments DSH funds exceeding hospital-specific DSH limits must be • repaid 12
CHASE Fee FFY 2017-18 CHASE Model • ➢ $896 million CHASE fees ▪ Net Patient Revenue at 5.75% of estimated NPR ➢ $1.27 billion in hospital supplemental payments ▪ Upper Payment Limit at 96.9% 13
CHASE Fee Net reimbursement reflects direct supplemental payments • minus total CHASE fees and does not include revenue received by hospitals due to expansion ➢ For comparison’s sake, data include fees and payments prior to July 1, 2017 under the Colorado Health Care Affordability Act (CHCAA) FFY 2017-18 Hospital Net Reimbursement 1 Fees / Payments 2014-15 2015-16 2016-17 2017-18 Total Supplemental $1,186,200,000 $1,120,800,000 $1,166,000,000 $1,266,400,000 Payments Total Fees $688,400,000 $670,000,000 $782,300,000 $896,300,000 Net Reimbursement $497,800,000 $450,800,000 $383,700,000 $370,100,000 to Hospitals rounding may cause calculation discrepancies 15
CHASE Fee Net reimbursement reflects direct supplemental payments • minus total CHASE fees and does not include revenue received by hospitals due to expansion For comparison’s sake, the 2016 -17 data reflects 12 months of • fees and payments, including fees and payments under the CHCAA from October 1, 2016 through June 30, 2017 and under CHASE from July 1, 2017 through September 30, 2017 FFY 2017-18 Net Hospital Reimbursement 1 Fees / Payments 2016-17 2 2017-18 Difference Total Supplemental $1,166,000,000 $1,266,400,000 $100,400,000 Payments Total Provider Fees $782,300,000 $896,300,000 $114,000,000 Net Reimbursement $383,700,000 $370,100,000 $(13,600,000) to Hospitals rounding may cause calculation discrepancies 16
CHASE Fee FFY 2017-18 Fees and Payments Expenditures Fees Federal Funds Total Funds IP Base Rate Supplemental Payment $228,900,000 $228,900,000 $457,700,000 OP Supplemental Payment $214,000,000 $214,000,000 $428,000,000 Uncompensated Care Supplemental Payment $55,200,000 $55,200,000 $110,500,000 DSH Supplemental Payment $86,300,000 $86,300,000 $172,600,000 HQIP Supplemental Payment $48,800,000 $48,800,000 $97,600,000 Total Supplemental Payment $633,200,000 $633,200,000 $1,266,400,000 Medicaid Parents to 133% of FPL $29,800,000 $280,500,000 $310,300,000 Medicaid Adults without Dependent Children to 133% of FPL $101,800,000 $1,625,200,000 $1,727,000,000 Medicaid Buy-In for Working Adults and Children with Disabilities $33,100,000 $36,800,000 $69,800,000 CHP+ 206% to 250% of FPL $8,600,000 $55,300,000 $64,000,000 Twelve Months Continuous Eligibility for Medicaid Children $31,300,000 $31,300,000 $62,600,000 Non Newly Eligibles $8,600,000 $42,500,000 $51,000,000 Medicaid Expansion $213,200,000 $2,071,700,000 $2,284,900,000 Administration $26,800,000 $49,100,000 $75,900,000 Transfer to General Fund – 25.5-4-402.4 (5)(b)(VII) $15,700,000 *$0 $15,700,000 Total Other Expenditures $42,500,000 $49,100,000 $91,600,000 Cash Fund Reserve $8,600,000 $0 $8,600,000 Grand Total $896,300,000 $2,754,400,000 $3,650,900,000 rounding may cause calculation discrepancies *Federal funds drawn from the transfer to the General Fund are not shown 17
Return on Investment $896 million generates $2.75 billion in federal funds, a • 207% return on investment Administrative expenditures ($75.9 million) are 2.1% of total • CHASE expenditures ($3.65 billion) Administrative expenditures include the following • ➢ Staff costs, legal services, accounting, etc. ➢ Contracted services, including utilization management and external quality review ➢ IT systems (i.e. eligibility and claims) and staffing for the customer contact center for more than 500,000 covered lives 18
CHASE Fee Inpatient fee assessed on managed care and non-managed • care days ➢ Inpatient fee ▪ Per non-managed care day: $391.15 ▪ Per managed care day: $87.52 Outpatient fee assessed on percentage of total Outpatient • charges ➢ Outpatient fee ▪ Percentage of total charges: 2.0208% 19
CHASE Fee Psychiatric, long term care, and rehabilitation hospitals are fee • exempt Certain hospitals receive a discounted fee • ➢ Inpatient fee ▪ High Volume Medicaid & CICP hospitals discounted 47.79% ▪ Essential Access hospitals discounted 60% ➢ Outpatient fee ▪ High Volume Medicaid & CICP hospitals discounted 0.84% 20
CHASE Fee CHASE Fee Calculation Row Description Amount Calculation Row 1 Managed Care Days 5,000 Row 2 Fee Per Managed Care Day $100.00 Row 3 Managed Care Day Fee $500,000 Row 1 * Row 2 Row 4 Non-Managed Care Days 10,000 Row 5 Fee Per Non-Managed Care Day $350.00 Row 6 Non-Managed Care Day Fee $3,500,000 Row 4 * Row 5 Row 7 Total Inpatient Fee $4,000,000 Row 3 + Row 6 Row 8 Total Outpatient Charges $50,000,000 Row 9 Fee Percentage 1.5000% Row 10 Total Outpatient Fee $750,000 Row 8 * Row 9 Row 11 Total Fee $4,750,000 Row 7 + Row 10 Your hospital’s calculation can be found on Page 7 (Table 4 & Table 5) of the June 14, 2018 letter 21
CHASE Fee Payers include: Fee exempt: CHASE Fees ✓ General Acute ✓ Rehabilitation $896 million ✓ Critical Access ✓ Long Term Care ✓ Pediatric ✓ Psychiatric IP NPR Limit OP NPR Limit IP Fee OP Fee $424 million $473 million Days Charges 22
Supplemental Payments Inpatient Base Rate Medicaid Supplemental Payment • Outpatient Medicaid Supplemental Payment • Uncompensated Care Medicaid Supplemental Payment • Disproportionate Share Hospital (DSH) Supplemental Payment • Hospital Quality Incentive Payment (HQIP) Medicaid • Supplemental Payment 23
Inpatient Base Rate Supplemental Payment Increase rates for inpatient hospital services for Medicaid • members Total Payments: $457.7 million • Inpatient Base Rate Payment = Medicaid rate before add-ons • times inpatient percentage adjustment factor times estimated Medicaid discharges times case mix 24
Inpatient Base Rate Supplemental Payment Inpatient Base Rate Supplemental Medicaid Payment Calculation Row Description Amount Calculation Medicaid Rate Before Add-ons Row 1 $6,000 Percentage Adjustment Factor Row 2 50% Incremental Medicaid Rate Bf Add-ons Row 3 $3,000 Row 1 * Row 2 Estimated Medicaid Discharges Row 4 1,000 Case Mix Row 5 1.05 Row 6 Total Payment $3,150,000 Row 3 * Row 4 * Row 5 Your hospital’s calculation can be found on Page 8 (Table 6) of the June 14, 2018 letter 25
Outpatient Supplemental Payment Increase rates for outpatient hospital services for Medicaid • members Total Payments: $428 million • Outpatient Payment = estimated Medicaid outpatient cost • times outpatient percentage adjustment factor 26
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries