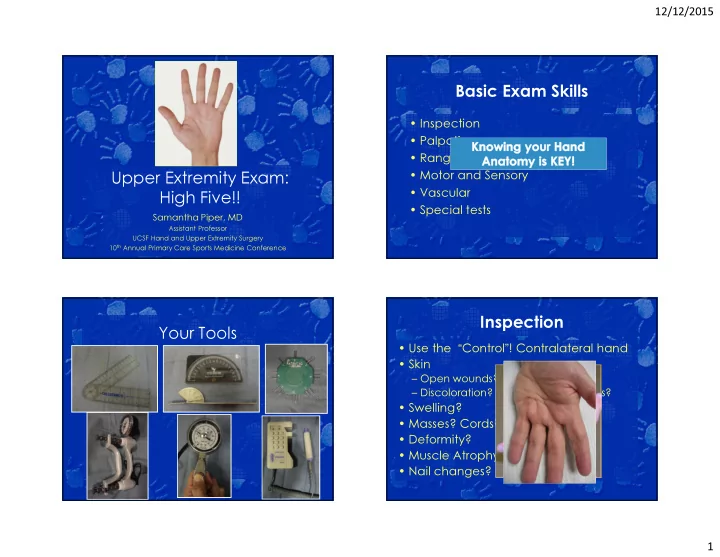
12/12/2015 Basic Exam Skills • Inspection • Palpation • Range of Motion • Motor and Sensory Upper Extremity Exam: • Vascular High Five!! • Special tests Samantha Piper, MD Assistant Professor UCSF Hand and Upper Extremity Surgery 10 th Annual Primary Care Sports Medicine Conference Inspection Your Tools • Use the “ Control ” ! Contralateral hand • Skin – Open wounds? Scars/marks? – Discoloration? Redness? Ecchymosis? • Swelling? • Masses? Cords? • Deformity? • Muscle Atrophy? • Nail changes? 1
12/12/2015 Inspection • Digital cascade/resting posture? Open wounds Inspection: What lies beneath? Surface Landmarks • Location of wound + knowledge of surface anatomy = – Accurate assessment of potentially injured structures •Distal perfusion? – Pulses, color, cap refill, temperature •Distal sensation and motor function? •Tendon continuity? – Cascade, tenodesis, active movement •Bone or joint injury? 2
12/12/2015 Palmar Landmarks • Name the creases Kaplan’s Cardinal Line 3
12/12/2015 ~6mm ~1cm Flexor Surface Markers Dorsal Landmarks 4
12/12/2015 Extensor Landmarks Palpation • Local Tenderness? – One finger • Abnormal bony anatomy? A1 Pulley: Trigger MPJ: OA • Masses? • Joint effusion? Crepitus? • Pulses? MP UCL CMC: Carpal Boss • Temperature? 5
12/12/2015 Radial Styloid- Dequervain’s Thumb CMC Scaphoid Scaphoid- Tubercle Snuffbox Scapho-styloid Joint Proximal Pole Lister’s 6
12/12/2015 Hook of Hamate SLJ Lunat LT Joint PT Joint e Fovea DRUJ ECU Lister’s Range of Motion Testing Tendons • Active & Passive • Tenodesis effect Extension Flexion • Is it limited? Why? Forearm P 70 S 85 – Swelling? Wrist 70, RD 20 75, UD 35 – Bone, Tendon, Nerve or Joint injury? MP 0- +45 90 – Arthritis? Disease? PIP 0 100 DIP 0 80 • Record the range of motion! Thumb MP +10 55 – Each Joint Thumb IP +15 80 – Total Arc Motion (TAM) Thumb CMC PA 0 45 – Distance to Palmar Crease (DPC) Thumb CMC RA 0 60 7
12/12/2015 FDS FDP & FPL • Immobilize FDPs Terminal Tendon Central Slip • Elson Test – PIP flexed 90* – Pt attempts to extend PIP – Assess DIP tension •Lax- CS intact •Tight- CS out 8
12/12/2015 Upper Limb Neurologic Strength Examination • Test both hands, mean of 3 trials • Compression neuropathy- Always – Grip check the C-spine! •5 adjustable hand spacings •Rapid alternating • Three major nerves – Pinch – Median •Tip- M – Ulnar •Key- M&U – Radial Cervical Radiculopathy Two Point Discrimination • Innervation density • ROM in 3 planes (F/E, lateral F, Rot.) • Objective – Pain or radicular radiation • Test both sides of finger – different nerves • TTP along C-spine • Normal < or = 5 mm • Spurling’s Thumb/Index/Long/Ring/Small • Axial Compression 5/5/5/5/7 5r8u/7r5u/5/5/5 9
12/12/2015 Median nerve - Motor Median nerve – Extrinsic Motor • “ OK ” sign • Extrinsic muscles : Origin in Forearm • AIN - Anterior Interosseous n. – PT, FCR, PL – 4 FDS, 2 FDP (index & long) – FPL, PQ No DIP flexion! • Intrinsic muscles - Located in Hand – Thenars (APB, FPB, Opp) – Lumbricals I, II OK! Not OK! Best Median Sensory Median nerve – Intrinsic Motor – “ Make an L with your thumb ” • Opposition Best Test Common and Proper Palpate here - Feel the * digital nerves Abductor Pollicis Brevis Palmar cutaneous nerve 10
12/12/2015 Ulnar nerve - Motor Ulnar nerve – Extrinsic Motor • Extrinsic – forearm origin – FCU Small finger DIP flexion - FDP – 2 FDP (ring & small) • Intrinsic – located in the hand – Hypothenars (ADM,FDM, ODM) – Lumbricals III & IV – Dorsal and palmar interosseous – Adductor Pollicis – Deep head FPB Ulnar nerve – Intrinsic Motor Ulnar nerve- Intrinsic Motor • Wartenberg’s Sign – Unopposed EDM (rad) due to loss of intrinsics Hypothenar m. 1st dorsal interosseous m. Palpate here 11
12/12/2015 Ulnar intrinsic motor • “ Claw ” deformity – “ intrinsic minus ” Ulnar nerve lesion • Froment ’ s sign – Substitute FPL for adductor PIP Flexion Hyperextension of MP Best Ulnar Sensory Radial nerve - Motor • All Extrinsic – from forearm • Wrist, finger and thumb extension • EPL: Retropulsion • PIP extension is Common and Proper digital nerves intrinsic function – Median/ ulnar 12
12/12/2015 Best Radial Sensory Digital Vascular Exam Dorsal branches of proper digital • Allen test nerves supply these areas • Doppler US of finger • O2 Sat Probe- should be NORMAL Carpal Tunnel Syndrome • Tinel ’ s sign Special Tests by Diagnosis • Phalen ’ s test • Durkin’s carpal compression test 13
12/12/2015 Phalen ’ s test Tinel’s Hold for 60s or until Sxs Increases pressure on median nerve • Tap along course of nerve – Positive if tingling in nerve distribution Positive if patient reports numbness in median distribution Durkin’s Compression test Cubital Tunnel Syndrome Hold for 30s or until Sxs • Tinel’s Sign • Flexion compression test • Ulnar nerve subluxation Positive if patient reports numbness in median distribution 14
12/12/2015 Ulnar Nerve Flexion Thumb CMC Arthritis Compression Test • Grind test – stresses joint Hold for 30s or until sxs – Positive if painful Positive if patient reports numbness in median distribution Thumb CMC Arthritis Thumb CMC Arthritis • Gelberman Adduction test – • Shoulder sign stresses joint – Positive if painful • MP Hyperextension – >30* is pathologic 15
12/12/2015 Wrist Thumb & Finger MP CL tear Radial Ulnar • Varus and Valgus Stress test • Dequervain’s • DRUJ Instability – Thumb: 0 & 30* flexion – Finkelstein’s – Piano Key – Digit: 0 & 90* – Shuck • SL Ligament Positive if >30* angulation, no endpoint, or gross • Ulnar Impaction/TFCC – Watson’s Shift laxity compared to contralateral side – Ulnar carpal abutment • Ganglion Cyst • LT Ligament – Trans illumination – LT ballottement • Scaphoid injury/SLAC/SNAC • ECU Pathology – Subluxation – Synergy DeQuervain ’ s tenosynovitis SL Stability Finkelstein ’ s test • Watson Shift test Pain here! Positive if asymmetrical click or if patient reports pain at DORSAL SLJ 16
12/12/2015 Ganglion Cysts DRUJ Instability • Trans illumination • Piano Key • Don’t forget Allen’s if volar radial wrist! Positive if increased laxity compared to contralateral side DRUJ Instability Ulnar Impaction/TFCC • Shuck • Ulnar carpal abutment stress test – Check in •Neutral •Supination •Pronation Positive if increased laxity compared to contralateral side 17
12/12/2015 ECU Pathology ECU Pathology • ECU Stability – Palpate ECU at ulnar groove through forearm • ECU Synergy Test ROM – Resisted finger abduction • Subluxates with Supination, Flexion, & UD • Reduces with pronation – Positive if pain over – Positive if ECU felt subluxating out of groove, ulnar wrist popping. • Resisted wrist extension and UD – Pain indicated ECU pathology Medial/Lateral Epicondylitis • Resisted wrist F/E with elbow Thank You! extended – Positive if pain at M/L elbow 18
12/12/2015 Inspection: Carrying Angle Normally:10* in men; 15* in women ELBOW varus valgus deformity deformity Inspection: Lateral Inspection • Posterior – Olecranon bursa • Medial – Subluxation of ulnar nerve 19
12/12/2015 Bony Palpation Inspection: Symmetry Bony Palpation Bony Palpation 20
12/12/2015 Bony Palpation Soft Tissue Palpation Pronation/supination ~80/~80 Range of Motion Compare to opposite side Flexion >135 Keep elbows against flanks to block Extension 0 or more shoulder compensation Compare to opposite side 21
12/12/2015 Functional Motion Neurologic Exam: Motor • Functional range E/F = 30-130* • Flexion: Brachialis, biceps (musc. n., C5,C6) – Loss of flexion more disabling than • Extension: Triceps (radial n., C7) loss of extension • Supination: Biceps, supinator (radial n., C6) • Pronation: Pronator teres (med. n., C6), • Functional range P/S = 50-50* pronator quadratus (ain, C8, T1) C5 Neuro Neuro Exam: Exam: Reflexes Sensation C6 T1 • Biceps - C5 • Brachioradialis – C6 C8 • Triceps – C7 C7 22
12/12/2015 ‘ Hook Test ’ for distal Special Tests O ’ Driscoll et al, AJSM 2007 biceps • Tennis elbow stress Ligament Stability Lateral pivot shift test (O'Driscoll/Morrey JBJS 73A:440,1991) • Supine • Extension • Supination • Valgus stress • Axial load Apprehension or shift = ++ Subluxed in extension and reduces as you flex past 40-60 degrees 23
12/12/2015 Pushup sign Chair sign ‘ Moving Valgus Stress Test ’ for Milking maneuver for MCL MCL - • Positive test is a subjective apprehension, instability, or • Create a valgus stress by pulling on the patient's thumb with the pain at the MCL origin between 70 & 120 degrees forearm supinated and elbow flexed at 90 degrees • 100% sensitive and 75% specific • Positive test is a subjective apprehension, instability, or pain at the MCL origin O ’ Driscoll et al, AJSM 2007 24
12/12/2015 Thank You! 25
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries