
Knee Physical Exam and Disclosures: None Injection Skills Carlin - PDF document
Knee Physical Exam and Disclosures: None Injection Skills Carlin Senter, MD Henry Crevensten, MD Associate Professor Associate Professor of Medicine, UCSF Primary Care Sports Medicine Deputy Director Primary Care UCSF Medicine and
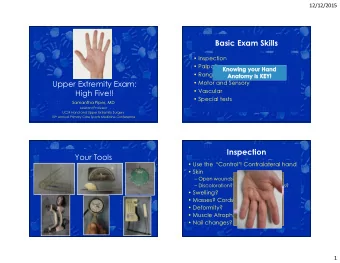
Knee Physical Exam and Disclosures: None Injection Skills Carlin Senter, MD Henry Crevensten, MD Associate Professor Associate Professor of Medicine, UCSF Primary Care Sports Medicine Deputy Director Primary Care UCSF Medicine and Orthopaedics San Francisco VA Health Care System UCSF Essentials of Women’s Health 7/2/19 2 Presentation Title 2 tendons 4 bones Knee Anatomy 3 articular surfaces 4 ligaments 2 menisci
3 articular surfaces 4 ligaments PCL LCL MCL ACL Articular cartilage 2 menisci (or meniscuses) Musculoskeletal work-up H istory Medial and lateral • I nspection • Shock absorber • Stabilizer P alpation R ange of motion O ther T ests
Most common knee problems in US adults Common causes of knee pain by location of Patellofemoral pain Meniscus tear OA symptoms syndrome (PFPS) Anterior Medial Age Younger Young- middle age Older or h/o - Patellofemoral syndrome - Joint line: meniscus tear or OA trauma Activity Overuse injury Acute or degenerative Acute or overuse - Quadriceps tendinitis - MCL sprain - Patellar tendinitis - Pes anserine bursitis Swelling Soft tissue (no effusion) +/- effusion +/- effusion If torsional instability think ligament tear. - Patellar / quad tendon tear Posterior Locking May endorse but usually If bucket handle tear May endorse but Lateral - Hamstring tendinitis crepitus usually crepitus - Joint line: meniscus tear or OA - Gastrocnemius strain Instability Pain may lead to this Not usually Preceded by pain - IT band syndrome - Meniscal root tear esp. down hills/ stairs - LCL sprain (rare) - OA, meniscus tears, effusion, popliteal cyst…. The essential knee exam To identify patellofemoral pain, OA and meniscus tears Standing: Inspection (varus, valgus or neutral) Seated - Palpation of joint lines (and in doing so palpating distal femur, proximal tibia) The essential knee exam - Examine for quad atrophy (by having patient straighten legs, compare side to side) Supine - Palpation of patellar facets Bonus maneuvers - supine - Evaluate for effusion 1. Lachman (ACL) - Range of motion: flexion, extension 2. Valgus stress (MCL) 3. Varus stress (LCL) - McMurray test (meniscus) 4. Posterior drawer (PCL) Standing: Squat and Thessaly tests (meniscus)
Standing: Inspection Seated: Joint line tenderness (JLT) Femur Lateral joint line Medial joint line Tibia Fibula Patella Medial: Sensitivity 83%, Specificity 76% Lateral: Sensitivity 68%, Specificity 97% http://doctorhoang.wordpress.com/ http://www.kneereplacementlondon.com/patient- 2010/09/06/valgus-knee-and- information/osteotomy bunion/ Konan et al. Knee Surg Traumatol Arthrosc. 2009 Supine: Palpation of patellar facets Effusion Video courtesy of Dr. Anthony Luke
Knee range of motion Meniscus: McMurray test Sensitivity medial 65%, Specificity medial 93% T est for meniscus: ROM: normal 0-135 - Determine if knee is locking or if Internally rotate the tibia and ROM is limited due to effusion extend lateral meniscus and/or pain/guarding/stiffness - Locking: think bucket handle Externally rotate the tibia and meniscus. extend medial meniscus Urgent xrays, MRI Pain and / or snap/click at the Urgent referral to sports joint line = concerning for surgeon for arthroscopy meniscus tear Magee, DJ. Orthopaedic Physical Assessment, 5 th ed. 2008. Video courtesy of Dr. Anthony Luke Composite exam: JLT + McMurray Lachman test for ACL Sensitivity 75-100%, specificity 95-100% JLT more sensitive than McMurray for meniscus tear This is a McMurray more specific than JLT for meniscus tear negative Lachman test: Joint line tenderness LR 0.9 for positive exam there is an McMurray LR 1.3 for positive exam endpoint to Composite assessment LR 2.7 for positive exam the anterior tibial translation. Solomon DH et al. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee? JAMA. 2001 Oct 3;286(13):1610-20. Magee, DJ. Orthopaedic Physical Assessment, 5 th ed. 2008.
Positive Lachman Valgus stress for MCL and Varus stress for LCL This is a normal exam (no pathologic laxity). Video courtesy of Drs. Kalli Hose and Anna Quan Posterior drawer for PCL Standing: Meniscus: squat Patient stands flat-footed Examiner holds their hands for balance Patient squats as low as possible (+) If pain or feeling of locking while knees bent Sensitivity 75-77%, Specificity 36-42% Snoeker BAM et al. J Orthop Sports Phys Ther. 2015 Sep;45(9):693-702.
Standing: Meniscus: Thessaly test If medial pain when pivot medially then How to do a Knee concern for Injection medial meniscus tear; if lateral pain when pivot laterally then concern for lateral Carlin Senter, MD meniscus tear. Associate Professor Primary Care Sports Medicine University of California San Francisco Video courtesy of Dr. Anthony Luke Watch: How to do a Knee Injection Video Indications for knee aspiration/injection https://binged.it/2QCSWcw Diagnostic - Effusion, esp atraumatic - Send for cell count, differential, crystals +/- gram stain and culture Therapeutic - Osteoarthritis - Crystal arthropathy - Inflammatory arthritis
Contraindications to steroid injection Intra-articular corticosteroid injections: benefits Short-term pain relief (6 weeks average) Joint infection Small effect on function Hemarthrosis No evidence for long-term pain relief Overlying cellulitis Clinical effect independent of degree of inflammation present Fracture - Don’t need to restrict injection just to those with effusion Frequency: general practice once every 3-4 months max Prosthetic joint - Concern for cartilage toxicity if given q 3 months x 2 years Risks of steroid injection in the knee Relative contraindications to steroid injection Corticosteroid injection within past 3-4 months Diabetics: increased blood sugar, 300 mg/dl starting as early as 2 hours after, lasting 5 days Facial flushing: 10% with Kenalog Coagulopathy - 19-36 hours post-injection Skin or fat atrophy Poorly controlled diabetes Post-injection steroid flare: 1-10% - Synovitis in response to injected crystals - Within hours - 48 hours post-injection - More common in soft tissue injections (20% of trigger points) than intra-articular injections Septic arthritis: 1/3000-1/50,000 - 1-2 days after injection Habib GS. Clin Rheumatol, 2009. UpToDate, “Joint aspiration or injection in adults,” 2010.
Why aspirate the effusion before injection? Aspiration/injection supplies Betadine swab x 3 • Clinically Ethyl chloride spray • - Decreased pain and stiffness because effusion gone - More effect of steroid because not diluted by effusion Alcohol swabs x 6 • - Inspect fluid for inflammation/infection, send to lab if question 4x4 gauze x 1 • - Confirms that injxn was intra-articular Bandaid x 1 • Significantly greater improvement in VAS for patients who had joint aspirated at time of injection in knee OA patients (Gaffney K et al, Ann Rheum Dis, 1995.) Reduction in relapse for 6 months after injection in RA patients (Weitoft T et al, Ann Rheum Dis, 2000.) Needles, syringes, meds Aspiration
Superolateral approach Post-injection patient instructions Patient supine Rest: no definitive evidence-based recommendation Extend knee - Recommendations in literature vary Bump under knee so flexed 10-20 No restrictions degrees Bed rest x 24 hours Light activity x 7 days, no weight bearing exercise Superior border patella - I recommend no strenuous activity x 7 days Lateral border patella Avoid swimming, hot tub, bath x 24 hours 1cm below - Let injection site heal Mark with syringe cover or tip of pen
UCSF CME: Essentials of Women’s Health July 2019 The Essential Physical Exam of the Knee for the Primary Care Clinician Maneuver Notes Standing Inspection (knees varus, valgus, neutral, feet pronated or supinated) Supine Palpate patellar facets Evaluate for effusion Range of motion (flexion, extension) McMurray’s test (meniscus) Supine or Seated: bonus maneuvers Valgus stress for MCL at 0 and 30 degrees Varus stress for LCL at 0 and 30 degrees Lachman test for ACL Posterior drawer for PCL Standing Squat (meniscus) Thessaly (meniscus)
Shoulder Physical Exam and Disclosures: None Injection Skills Carlin Senter, MD Henry Crevensten, MD Associate Professor Associate Professor of Medicine, UCSF Primary Care Sports Medicine Deputy Director Primary Care UCSF Medicine and Orthopaedics San Francisco VA Health Care System UCSF Essentials of Women’s Health 7/2/19 2 Presentation Title Shoulder bony anatomy Clavicle SC joint AC joint 3 bones: -clavicle -scapula Shoulder anatomy -humerus Humerus 4 joints: Scapula -acromioclavicular Glenohumeral -glenohumeral joint -scapulothoracic -sternoclavicular Slide adapted with permission from Drs. Meg Pearson and Steve Bent
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.