Ac c e le r ating He alth Syste m T r ansfor mation Wha t ro le fo r ACOs? Ho w mig ht we do b e tte r? Ove r vie w Conc e ptua l fra me work: wha t a re we trying to a c hie ve ? Whe re a re we now? Na tio na l po lic y c o nte xt • Wha t do we kno w a b o ut ACO c a pa b ilitie s? • Wha t do ACOs think is impo rta nt? • Wha t role for c e rtific a tion? Wha t e lse mig ht we do? Moving forwa rd
Conc e ptual F r ame wor k Wha t a re we trying to a c hie ve ? Purpose : improve c a re , improve he a lth, lowe r c osts F o r pa tie nts se rve d b y he a lth syste ms • F o r a ll re side nts o f c o mmunitie s the y se rve • Sourc e s of le ve ra g e F ina nc ia l inc e ntive s • Re g ula tio n • Pe rfo rma nc e me a sure me nt / pub lic re po rting • L e a rning / fe e db a c k / te c hnic a l suppo rt •
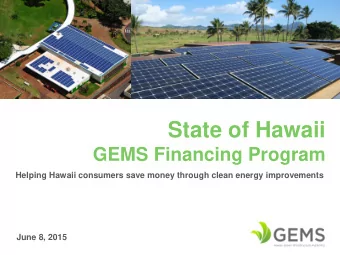
Whe r e ar e we now? Na tio na l Po lic y Co nte xt ACO pa yme nt mode l c ontinue s to e xpa nd 749 ACOs (F e b rua ry) • Physic ia n Gro up: 295 Go ve rnme nt 404 Ho spita l le d: 314 Co mme rc ia l 220 I nsure r 54 Bo th: 104 Number of Enrollees (Millions) Sources: Kaiser Family Foundation; Leavitt Partners
Whe r e ar e we now? Na tio na l Po lic y Co nte xt E a rly e vide nc e : g la ss ha lf full Qua lity • ACO syste ms pe rfo rming b e tte r tha n F F S (se le c tio n) ACOs impro ving o n a lmo st a ll me a sure s (se le c tio n le ss like ly) Co st: mo de st sa ving s (MSSP, Pio ne e r, AQC) • Co ntrib uting to slo wing o f Me dic a re spe nding g ro wth? • Me dic a id ACOs a ppe a r pro mising • E a rly e vide nc e : g la ss ha lf e mpty Me dic a re : ha lf a c hie ve d sa ving s; o ne q ua rte r g o t b o nus • Ma jo r c o nc e rns a b o ut MSSP a nd Pio ne e r • F ina nc ia l mo de l to o unpre dic ta b le ; to o little e a rly re turn Diffic ult fo r ACOs to e ng a g e pa tie nts (Me dPAC: 1/ 69) Ma ny still o n side line s; ma ny pla ying vo lume / pric e g a me •
Whe r e ar e we now? Na tio na l Po lic y Co nte xt F e de ra l c ommitme nt to moving forwa rd a ppe a rs strong Se c re ta ry Burwe ll’ s a nno unc e me nt • ACOs: 30% b y 2016; 50% b y 2018: CMS mo ving fo rwa rd • Re visio n o f MSSP rule unde rwa y Additio na l CMMI pro g ra ms like ly (“Va ng ua rd”? ) Priva te se c tor? He a lth Ca re T ra nsforma tion T a skforc e Purc ha se rs, Pa ye rs, Pro vide rs a nd Pa tie nts -- to g e the r • Co mmitme nt to 75% T riple -a im b a se d c o ntra c ts b y 2020 •
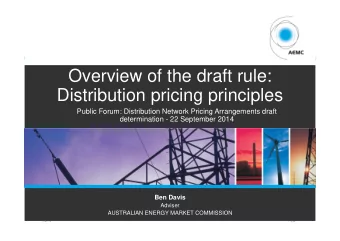
Whe r e ar e we now? ACO Ca pa b ilitie s ACO Char ac te r istic s Co mpre he nsive pre -visit pla nning , me dic a tio n 27% ma na g e me nt, & pre ve nta tive c a re re mind e rs Co mpre he nsive c hro nic c a re ma na g e me nt in 36% pla c e Ac tive ly e ng a g e s in p ro g ra ms to re d uc e ho spita l 62% a d missio ns fo r a mb ula to ry c a re se nsitive c o nd itio ns Syste ms in pa lc e to a ssure smo o th tra nsitio ns a c ro ss 25% c a re se tting s Ro utine ly a sse sse s ina ppro pria te use o f the E D a nd 47% use s this da ta to re d uc e use F ully de ve lo pe d p ro g ra m to a sse ss a nd re d uc e 46% ho sp ita l re a dmissio ns 0% 10% 20% 30% 40% 50% 60% 70% Proportion of ACOs
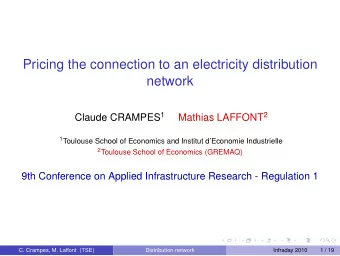
Whe r e ar e we now? ACO Ca pa b ilitie s Use of Physic ian Pe r for manc e Manage me nt Str ate gie s 90% 77% 80% Pe rc e nt Pa rtic ipa tion 70% 59% 60% 50% 50% 40% 40% 30% 23% 20% 8% 10% 0% No ne I ndividua l I ndividua l Co st One -o n-o ne I ndividua l I ndividua l no n- Qua lity Me a sure s re vie w a nd fina nc ia l fina nc ia l Me a sure s fe e d b a c k inc e ntive s re wa rds o r re c o g nitio n
Whe r e ar e we now? Wha t do we kno w a b o ut wha t ACOs think is impo rta nt? ACO Re a dine ss T ool – Orig ins De ve lo pe d with he a lth syste m e xe c utive s • He lp the m a nswe r q ue stio n: “Wha t sho uld I do ? ” • Co nte nt: NSACO, AMGA, e xe c utive s unde r APMs • Prio ritie s: “Ho w impo rta nt is this to suc c e ss? ” Co mpe te nc y: “Ho w a re yo u do ing o n this? ” Ga ps a re info rma tive : • Be twe e n prio ritie s a nd se lf-a sse sse d c o mpe te nc y Be twe e n e xe c utive s a nd fro nt-line pro vide rs Da ta now inc lude s 14 syste ms • T wo Pio ne e rs •
Whe r e ar e we now? Wha t do we kno w a b o ut c urre nt pe rc e ptio ns o f prio rity fo r va lue -o rie nte d Do ma ins? Pione e r A Pione e r B 106 T otal Re sponde nts 56 T otal Re sponde nts
Whe r e ar e we now? Wha t do we kno w a b o ut c urre nt pe rc e ptio ns o f pro fic ie nc y fo r va lue -o rie nte d Co mpe te nc ie s? Ave ra g e profic ie nc y sc ore s (1- 9) for two Me dic a re Pione e r ACOs. Bubble size indicates level of agreement across respondents – a bigger bubble indicates a wide variation in responses
Whe r e ar e we now? Wha t do we kno w a b o ut c urre nt pe rc e ptio ns o f prio rity fo r va lue -o rie nte d Do ma ins? Ave ra g e priority sc ore s (1- 5) for two Me dic a re Pione e r ACOs. Bubble size indicates level of agreement across respondents – a bigger bubble indicates a wide variation in responses
Ac c e le r ating He alth Syste m T r ansfor mation Ce rtific a tio n: Ge ne ra l tho ug hts Cha lle ng e s: Curre nt e vide nc e o n link b e twe e n c a pa b ilitie s a nd • pe rfo rma nc e is thin E xc e ptio ns: • L e a de rship: e sse ntia l (b ut ha rd to re g ula te ) I nsura nc e o ve rsig ht if risk b e a ring Pe rfo rma nc e re po rting (so we kno w ho w the y a re do ing ) Co nte xt matte rs – o rg a niza tio na l a nd ma rke t le ve l • Re ma rka b le dive rsity in c urre nt mo de ls Ove r- spe c ific a tion like ly ha rmful Re duc e s like liho o d o f inno va tive mo de ls e me rg ing • Pre c lude s le a rning fro m va ria tio n •
Ac c e le r ating He alth Syste m T r ansfor mation Ce rtific a tio n: Minimum sta nda rds, ACO L e ve l 1 Wha t I would hope for: Alig n with MSSP to e xte nt po ssib le • E nc o ura g e syste ms to mo ve to a ll-pa ye r ACO c o ntra c ts Minimize b urde n o f sta rting do wn APM pa thwa y • Allo w fle xib ility, inno va tio n, le a rning • L e g isla tive la ng ua g e se e ms c le a r ACO must re po rt ho w the y a re me e ting re q uire me nts • Avo id spe c ifying e xa c tly ho w (wo uld a llo w fle xib ility) • Conside r: Sta nda rdize d re po rting o n struc ture , c o ntra c ts, c a pa b ilitie s • (Ag a in – to suppo rt le a rning ) •
Ac c e le r ating He alth Syste m T r ansfor mation Ce rtific a tio n: Pro g re ssio n to hig he r le ve ls Wha t is the purpose of L e ve ls 2 a nd 3? Hig he r le ve ls o f risk b e a ring ? I nsura nc e re g ula tio n wise • Hig he r re wa rds? (re a so na b le ide a ) • Mo tiva tio n? (g o ld sta r? Suppo rt ma rke ting ? ) • A fe w thoug hts: L ink le ve ls to : • Pro po rtio n o f prima ry c a re pa tie nts unde r ACO mo de l De g re e o f risk b e a ring Ab ility to re po rt o n a dva nc e d me a sure s (PROMs, he a lth risk) Pric e re duc tio ns fo r re ma ining F F S c o ntra c ts Wha t mig ht a lte rna tive b e ? • T ranspare nc y o n pe rfo rmanc e Graduate d share d saving s
Ac c e le r ating He alth Syste m T r ansfor mation Spe c ific issue s Cross- c ontinuum ne twork Go a l: c o o rdina tio n, e ffe c tive tra nsitio ns, info rma tio n flo w Co nc e rn: wha t if b e st c a re is o utside ACO? Clinic a l inte g ra tion, pra c tic e g uide line s, E BM, pe rforma nc e improve me nt, popula tion he a lth ma na g e me nt I nfo rma tio n syste ms; risk stra tific a tio n, g a p a na lysis; te a ms Pro c e ss impro ve me nt (te a m); pro vide r fe e db a c k (individua l) Alig ne d inc e ntive s within ACO Pro po rtio n o f pa tie nts unde r APMs impo rta nt L ike ly va rie s b y site / pro vide r (PCPs vs Ho spita l vs po st-a c ute ) Ho w to e nc o ura g e re fe rra l o utside whe n b e tte r/ c he a pe r c a re Mig ht tra nspa re nc y he lp? (unit pric e )
What e lse might we do? L e ve ra g ing c e rtific a tio n pro c e ss to a c c e le ra te le a rning Sourc e s of le ve ra g e Re g ula tio n; fina nc ia l c e rtific a tio n Pa yme nt mo de l c o nc o rda nc e (push o the r pa ye rs) Pe rfo rma nc e me a sure me nt / pub lic re po rting L e a rning / fe e db a c k / te c hnic a l suppo rt How c e rtific a tion c ould he lp: De sig n the c e rtific a tio n pro c e ss to a c c e le ra te le a rning Sta nda rdize d da ta c o lle c tio n; link to pe rfo rma nc e tra c king Use a sse ssme nts to ide ntify pe e r-c o a c hing o ppo rtunitie s And: T e c hnic a l suppo rt (NAACOs); Ac c e ss to e vide nc e Da ta suppo rt;
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries