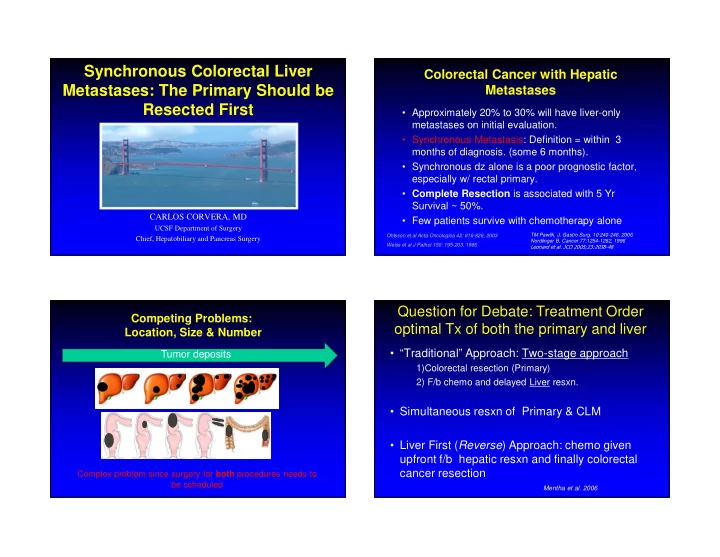
Synchronous Colorectal Liver Colorectal Cancer with Hepatic Metastases: The Primary Should be Metastases Resected First • Approximately 20% to 30% will have liver-only metastases on initial evaluation. • Synchronous Metastasis: Definition = within 3 months of diagnosis. (some 6 months). • Synchronous dz alone is a poor prognostic factor, especially w/ rectal primary. • Complete Resection is associated with 5 Yr Survival ~ 50%. CARLOS CORVERA, MD • Few patients survive with chemotherapy alone UCSF Department of Surgery Ohlsson et al Acta Oncologica 42: 816-826, 2003 TM Pawlik, J. Gastro Surg. 10:240-246, 2006 Chief, Hepatobiliary and Pancreas Surgery Nordlinger B, Cancer 77:1254-1262, 1996 Weiss et al J Pathol 150: 195-203, 1986 ���������������������������������� Question for Debate: Treatment Order Competing Problems: optimal Tx of both the primary and liver Location, Size & Number • “Traditional” Approach: Two-stage approach Tumor deposits 1)Colorectal resection (Primary) 2) F/b chemo and delayed Liver resxn. • Simultaneous resxn of Primary & CLM • Liver First ( Reverse ) Approach: chemo given upfront f/b hepatic resxn and finally colorectal Complex problem since surgery for both procedures needs to cancer resection be scheduled Mentha et al. 2006
Primary First vs Liver First Problems / Pitfalls of Traditional approach A. Treatment duration can be long (months ~3); risk dz progression in the liver progress beyond resection. B. Complications from Primary surgery: prevents delivery of systemic chemoRX in ~ 50 %. Sauer R, N Engl J. Med.2004;351:1731-1740 Ayez N, Dis Colon Rectum, 2013;56 (3):281-287 Data shows that the order doesn’t Matter! Bosset JF N Engl J Med 2006;355:1114-1123 Argument for Liver first approach? Resect Primary First A. Prognosis with synchronous disease is driven by the extent of liver metastases. • Primary tumor is large and near-obstructing. B. Pre-operative ChemRx is administered in > – Prevents local complications: Obstruction/bleeding. 80% patients. – Improves the intention-to-treat survival since ~ 80% • Liver First is associated with Dz recurrence ~ 25-67 % complete treatment. C. Biology is declared– Extrahepatic disease Survival data is Limited for the Liver First • approach = no difference in outcomes. would preclude resection. – Can avoid rectal surgery in patients who progress on chemotherapy. Sauer R, N Engl J. Med.2004;351:1731-1740 Ayez N, Dis Colon Rectum, 2013;56 (3):281-287
MD Anderson experience Retrospective Studies: N=156 Liver-First approach N= 72 N= 27 N= 43 Author N= Patients % 5 yr survival % Recurrence Brouquet 27 39 % 46 % De Jong 22 41% (3yr) 38 % Mentha 36 31 % 70 % De Rosa 37 30 % (3yr) 52 % Broquet et al, J Am Coll Surg 2010; 210:934-941 Mechteld, HPB 2011, 13,745-752 Mentha, Dig Surg 2008;25:430-435 Ayez, Dis Colon Rectum. 2013;56 (3):281-287 Broquet et al, J Am Coll Surg 2010; 210:934-941 Categories of Resectability Problems with Liver first approach A. Primary tumor can progress beyond resection Resectable dz by Unresectable but likely Initially unresectable and standard approach convertible with response unlikely convertible – Perforation or direct invasion BORDERLINE * B. Chemo responsiveness does not always persist. – Regrowth of “Disappearing” tumors * Extended approach Regrowth of Primary � Obstruction . – -Staged resections -Preop PVE C. Chemotherapy associated toxicity. -Resection plus RFA -ALPPS D. Disappearing Colorectal Primary. -Hepatic Arterial Infusion Pump
“Contemporary” Response to Chemotherapy Colorectal Liver Liver 2 nd stage Surgery Resection Dx Strategies SCLM Chemo Chemo Ch-XRT Recovery Recovery Completion Chemotherapy ChemoXRT Recovery Traditional/ Classical/ Historical Approach Colorectal Surgery Liver 2 nd stage & Liver (“easy” side) Dx SCLM Chemo Chemo Ch-XRT Recovery Completion Chemotherapy ChemoXRT Recovery Simultaneous/ Combined Approach Liver Resection Colorectal Liver 2 nd stage Surgery Dx SCLM First Line Chemo (3-6 cycles) Completion Recovery Chemo Ch-XRT Recovery Recovery Ch-XRT Chemotherapy “Reversed” or Liver First Approach Adam, Ann Surg 2004; 240:1052--61 Conclusions CONTACT INFORMATION: Carlos U. Corvera M.D. Associate Professor Department of Surgery • Hepatic resection remains critical to the long-term Gastrointestinal Surgical Oncology outcome of patients with synchronous colorectal Chief, Liver, Biliary and Pancreatic Surgery metastases. University of California, San Francisco School of Medicine Helen Diller Family Comprehensive Cancer Center • These patients are complex and should be managed by Email: carlos.corvera@ucsfmedctr.org Phone: Mobile # (415) 317-4602 multidisciplinary teams: Direct Line: (415) 502-1690 Clinic Line (referrals) Fax: (415) 353-9931 - Customized Treatments: individualized and based Tel: (415) 353-9888 on extent and location of disease, and tumor biology. Academic Address: Room U-370 - Prioritizing Tx should be based on the problematic 521 Parnassus Avenue component of the patient’s dz San Francisco, CA. 94143 Assistant (Marjorie Galicha) Management should be CHEMOTHERAPY-first and not email: Marjorie.Galicha@ucsfmedctr.org “Liver-first” tel: (415) 415-476-0762
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries