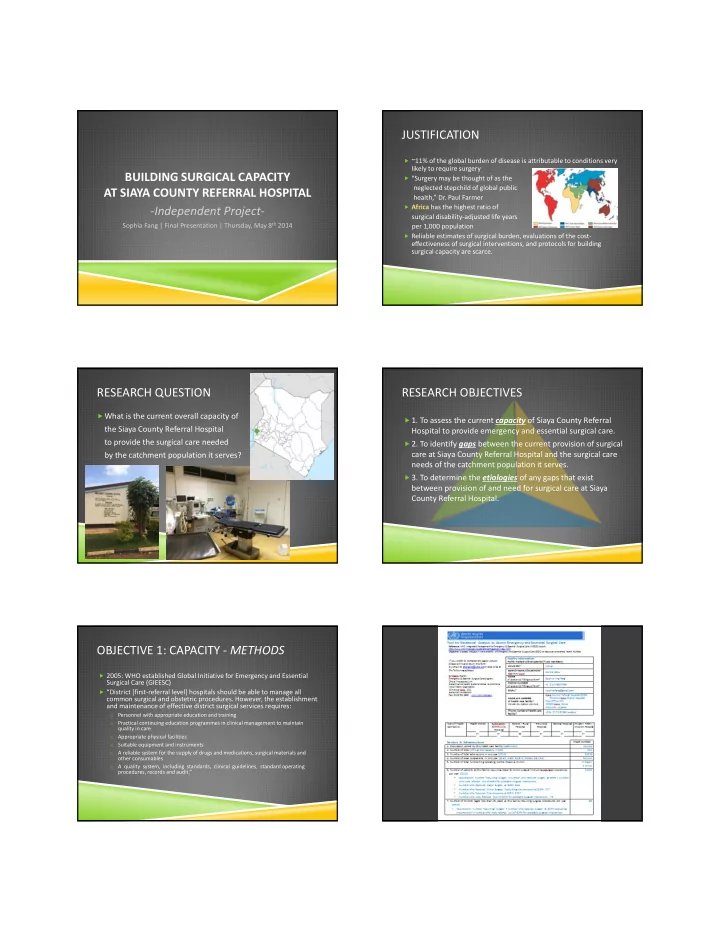
JUSTIFICATION ~11% of the global burden of disease is attributable to conditions very likely to require surgery BUILDING SURGICAL CAPACITY “Surgery may be thought of as the neglected stepchild of global public AT SIAYA COUNTY REFERRAL HOSPITAL health,” Dr. Paul Farmer Africa has the highest ratio of ‐ Independent Project ‐ surgical disability ‐ adjusted life years Sophia Fang | Final Presentation | Thursday, May 8 th 2014 per 1,000 population Reliable estimates of surgical burden, evaluations of the cost ‐ effectiveness of surgical interventions, and protocols for building surgical capacity are scarce. RESEARCH QUESTION RESEARCH OBJECTIVES What is the current overall capacity of 1. To assess the current capacity of Siaya County Referral the Siaya County Referral Hospital Hospital to provide emergency and essential surgical care. to provide the surgical care needed 2. To identify gaps between the current provision of surgical care at Siaya County Referral Hospital and the surgical care by the catchment population it serves? needs of the catchment population it serves. 3. To determine the etiologies of any gaps that exist between provision of and need for surgical care at Siaya County Referral Hospital. OBJECTIVE 1: CAPACITY ‐ METHODS OBJECTIVE 1: CAPACITY ‐ METHODS 2005: WHO established Global Initiative for Emergency and Essential “Tool for Situational Analysis to Assess Emergency and Essential Surgical Care” Surgical Care (GIEESC) Checklist of the infrastructure, human resources, interventions, and equipment and “District [first ‐ referral level] hospitals should be able to manage all supplies deemed necessary for a hospital to provide a basic level of surgical care common surgical and obstetric procedures. However, the establishment Successfully used to assess other hospitals in Kenya in cooperation with the MOH and maintenance of effective district surgical services requires: Modified Tool Personnel with appropriate education and training o to reflect Kenya’s medical training system Practical continuing education programmes in clinical management to maintain o additionally assess pediatric surgeries and ophthalmic surgeries quality in care Appropriate physical facilities => 7 ‐ page form with > 150 questions o Suitable equipment and instruments Completed Tool o A reliable system for the supply of drugs and medications, surgical materials and o With input from multiple staff members including medical superintendent, charge other consumables nurses, medical officers, clinical officers with higher diplomas in ophthalmology and A quality system, including standards, clinical guidelines, standard operating anesthesia o procedures, records and audit.”
OBJECTIVE 1: CAPACITY ‐ RESULTS OBJECTIVE 1: CAPACITY ‐ RESULTS Section A: Infrastructure Section B: Human Resources Catchment population: 43,124 Surgeons (qualified, i.e. consultant): Beds: 224 0 Obstetricians/Gynecologists (qualified): Total Admissions in 2013: 8,816 1 General doctors providing surgery (including obstetrics): 5 (medical officers) Total Outpatients in 2013: 52,411 Clinical officers providing surgery: Average patient travels 5 ‐ 20km to get to hospital ‐ boda boda 1 (ophthalmology) 2 Major + 2 Minor Operating Theatres Anesthetists: 2 (clinical officers) Water: plumbing throughout, supply unpredictable Nurses ‐ Theatre: 5 Electricity: daily outages with reliable back ‐ up Midwives: 56 Anesthesia Machines: 3 functional with continuous intraop vital monitoring Paramedics: 0 Inconsistent access to/use of management guidelines Engineers/Repair technicians 6 Access to Hgb/urine tests, x ‐ rays, blood but shortage of vital monitoring equipment outside theatre OBJECTIVE 1: CAPACITY ‐ RESULTS OBJECTIVE 1: CAPACITY ‐ RESULTS Section D: Emergency and Essential Surgical Care Equipment and Supplies Section C: Interventions Completely Lack: ✔ Most basic interventions without need to refer chest tubes Areas of Limitations: pediatric ‐ sized instruments Acute burn management Hernia Repairs (strangulated) Frequent Shortages: Laparotomy (intestinal obstruction, injuries) soap Neonatal and Congenital conditions eye protection Most non ‐ cataract ophthalmic surgeries tourniquets Orthopedic splints Resuscitator bag valve & mask (adults + peds) blood pressure measuring equipment for children catheters for children SIAYA VS. MOH LEVEL 4/5 STANDARDS SIAYA VS. MOH LEVEL 4/5 STANDARDS , cont. Level 4 Level 5 Siaya CRH Level 4 Level 5 Siaya CRH Minimum Human Resources Minimum Physical Infrastructure Medical Officers 6 15 5 Minor theatre in OPD 1 1 2 (at least 2 outpatient, 3 (at least 4 outpatient, 8 ENT services room in OPD 1 1 0 inpatient) wards, 2 maternity, 1 Laboratory 1 1 1 Operating theatre beds 2 4 (1 Gynae emergencies, 2 intensive care unit) 1 cold case, Anaesthesiologist 2 4 2 1 general emergencies, Nursing staff ‐ Theatre 10 40 5 1 ophthalmic) Nursing staff ‐ Intensive Care Unit 12 0 X ‐ ray room 1 1 1 (no ICU) Ultrasound room 1 1 1 ENT Clinical Officer 1 0 Source of running water, Yes Yes Yes but inconsistent Ophthalmology Clinical Officer 3 1 Water reservoir, Yes Yes Yes Water storage for roof Obstetricians/Gynaecologists 4 1 catchment Yes Yes Yes Surgeons 3 0 Generator house 1 1 1, reliable with several ‐ Ophthalmologists 2 0 minute delay in turning on ENT Specialist 1 0 Ambulance 1 1 2 Orthopaedic surgeon 1 0 Medical Engineering Unit Yes Yes
OBJECTIVE 2: GAPS ‐ RESULTS OBJECTIVE 2: GAPS ‐ METHODS Examination of handwritten logbook of General Surgery + OB/GYN + Ophthalmology + Circumcisions (ICAP) referrals in 2013 for Surgeries Needed by GAPS cases likely to require = 3480 Total Surgeries in 2013 n=255 Community surgical intervention. = 32.9% Hernias Transcribed all of the 17.3% Urology surgery cases done in 7.3% n=660 13.7% Orthopedics the main theatre in 66.7% Emergency C/S cs 3.3% Elective C/S Surgeries Surgeries 2013 as recorded in 3.8% Ectopic Provided by Provided by General Surgery Urgent Referrals Out the 3 handwritten 19.0% 24.8% Other OB/GYN Hospital Hospital logbooks: General OB/GYN Surgery, OB/GYN, Ophthalmology + Ophthalmology Circumcisions (ICAP) n=358 10.3% 63.4% 91.3% Cataract OBJECTIVE 2: GAPS ‐ RESULTS OBJECTIVE 3: CAUSES OF GAPS ‐ METHODS Total of 76 Referrals Out of Siaya County Referral Hospital in 2013 for Developed an 8 ‐ question survey to administer to hospital staff (goal Likely Surgical Interventions n=10 ‐ 15) involved in the care of surgical patients At least 75% of those cases were referred to Jaramogi Oginga Odinga Surveyed 33 staff members, including a consultant OB/GYN, medical Teaching and Referral Hospital (JOOTRH) in Kisumu (73.1 km) officers, clinical officers, anesthetists, and nurses working in the theatre, surgical wards, and maternity ward 15.8% 22.4% Traumatic Head Injury Traumatic Chest Injury Traumatic Fractures 3.9% Abdominal Other 38.2% 19.7% OBJECTIVE 3: CAUSES OF GAPS ‐ RESULTS OBJECTIVE 3: CAUSES OF GAPS ‐ RESULTS “Do you experience any constraints in caring for surgical patients?” “Do you refer any surgical cases to a higher ‐ level facility?” 78.8% of respondents circled “Yes” o 100% of respondents circled “Yes” o “What are the biggest problems experienced by Siaya District Hospital in o “If yes, what is the primary reason you refer?” (select 1 out of 6 choices) caring for surgical patients?” (rank top 5 out of 12 choices) 81.0% respondents chose “not enough consultant surgeons” as their #1 biggest 0.0% o problem 30.6% Top 5 Problems: o 47.2% Lack of surgical knowledge/experience 1. not enough consultant surgeons Lack of support staff 2. lack of equipment Lack of physical resources 8.3% Lack of diagnostics 3. not enough healthcare support staff (including nurses, clinical officers, etc.) 11.1% Lack of Intensive Care Unit 4. not enough anesthetists/anesthesiologists Patient preference 5. lack of diagnostics (labs, imaging, etc.) 2.8%
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries