#ctacQI CTAC Services in urban context Anne Mitchell Head of Older People & Primary Care Services, Glasgow City HSCP Derrick Pearce Head of Community Health Care Services, East Dunbartonshire HSCP
Community Treatment and Care Services Anne Mitchell – Head of Older People & Primary Care, Glasgow HSCP Derrick Pearce – Head of Community Health & Care Services, East Dunbartonshire HSCP 11 th June 2019
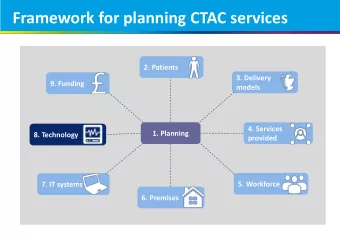
Context • NHSGG&C - 6 Partnerships – Diverse population • A whole NHSGG&C approach to ensure consistency for patients and for GP Practices • Delivering CTAC for 230 Practices across a predominantly urban setting but including rural outposts • Mixed model of delivery – some Partnerships have Treatment Room services fully embedded through to some who have none at all
Starting Point Position for Glasgow HSCP – Building on an existing model Variable access across the 3 localities Previous work to establish consistent processes • 43 rooms within 16 Health Centres • 40 registered staff & 10 unregistered staff • 3 band 6 co-ordinators within those numbers • Limited intervention list – dressings, leg ulcers, bloods, ears, injections • No scope for less mobile patients • No non medical prescribing / nurse led clinics
Position for East Dunbartonshire HSCP • East Dunbartonshire HSCP is least well developed • Starting from scratch – no current Treatment Rooms Service in place • All work currently undertaken by GP Practices or via Adult Community Nursing • No culture of shared services for GP Practices as a result of limited GP clustering in Health Centres
CTAC JOURNEY – current developments • Identify new accommodation • Recruitment timeline – Phased – induction programme – planning to do the above on board wide basis where possible • All registered nurses in a position to carry out micro suction ear care within 8 weeks (Glasgow) • Exploring hoist provision for non housebound patients (Glasgow) • Non medical prescribing – staff on v150 and v300 • In discussion with GCU re bespoke leg ulcer training • ECG Pilot project
Successes • Ear Care micro suction will reduce the number of nurse led appointments from 3 - 1 • ECG project will allow patients to be seen in Community rather than Hospital • Non medical prescribing will allow nurses to provide a nurse led service, efficient and beneficial for patients and reduce GP workload • Ambulant patients will be able to access services in the Community reducing the need for District Nursing calls and / or repeat visits to Practice
Challenges • Accommodation Issues • Liaison with Labs • IT to support • Exceptions – Practices & Patients • Appointing across a range of sites (choice) • GPs views on pace • Delivering consistency • Prescribing and supplies • Agreeing standard specification and working to that model • Treatment of children • Balancing phlebotomy with wider TR issues
What next • Expansion of Service as accommodation allows • Explore new interventions – eg catheter care, NG/Pegs, tracheostomy care etc • Roll out of ECG recording within City • Nurse prescribing • Developing A more Nurse Led service • Exploring innovative solutions to accommodation – including mobile • Working across into other areas and with acute
Any Questions?
Our Questions • Delivery Options – has anyone explored really innovative accommodation solutions? • Reflections/Options for full integration of CTAC staff into Adult Community Nursing – eg rotation? • Has anyone explored shared model with GP Practices eg using Practice staff with funding from HSCP/PC? • What do we see as the future developments within this workstream that we need to future proof for?
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries