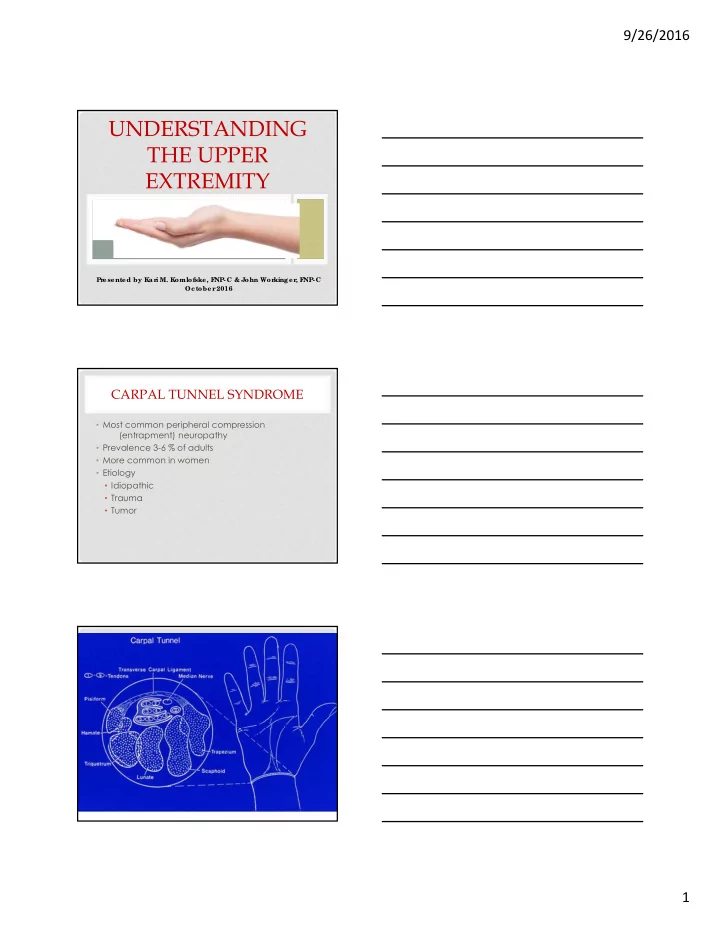
9/26/2016 UNDERSTANDING THE UPPER EXTREMITY Pr esented by Kar i M. Komlofske, F NP-C & John Wor kinger , F NP-C Oc tober 2016 CARPAL TUNNEL SYNDROME • Most common peripheral compression (entrapment) neuropathy • Prevalence 3-6 % of adults • More common in women • Etiology • Idiopathic • Trauma • Tumor 1
9/26/2016 CARPAL TUNNEL SYNDROME • Pain is NOT a primary symptom • Paresthesias (pins & needles) in palmar pads of digit tips, initially at night • Numbness (loss of sensation) (Semmes Weinstein monofilament testing) • Weakness of thumb abduction Loss of thumb dexterity (not grip) Wasting of thenar musculature CARPAL TUNNEL SYNDROME ASSOCIATED RISK FACTORS • Genetics • Hormonal factors • Pregnancy • Menopausal • Hypothyroidism • Obesity • Diabetes • Age • Gender • Rheumatoid arthritis • Occupation • Lozano-Calderon 2008 2
9/26/2016 CARPAL TUNNEL SYNDROME OCCUPATIONAL EXPOSURE • Keyboarding is NOT a risk factor • Evidence supports regular keyboarding is protective • Stevens 2001, Atroshi 2007, Mattioli 2009 • Vibration exposure • Barcenilla 2012 • Forceful & sustained heavy grip activities • Poultry/fish/meat processing • Palmer 2007, van Rijn 2009 CARPAL TUNNEL SYNDROME PHYSICAL EXAMINATION • Median nerve Tinel’s testing • Median nerve compression testing at wrist • Phalen’s maneuver • Weakness/wasting Abductor Pollicis Brevis • Sensibility testing with Semmes Weinstein monofilaments (index/little alone) CARPAL TUNNEL SYNDROME HISTORY CORRELATES WITH SEVERITY • Mild • Intermittent night time paresthesias • Moderate • Intermittent night time and day time symptoms to include numbness • Severe • Constant symptoms • Diminished protective sensation • Loss of thumb dexterity • Wasting of Abductor Pollicis Brevis 3
9/26/2016 WASTING OF ABDUCTOR POLLICIS BREVIS MUSCLE CARPAL TUNNEL SYNDROME Confirmatory Nerve Conduction Testing Required by CMS in Medicare/-aid patients prior to surgery No X-Rays needed CARPAL TUNNEL SYNDROME • Screen for hypothyroid and diabetes mellitus • 3-6 month trial of wrist bracing with mild, early symptoms • Consider corticosteroid injection if symptoms intermittent and no motor deficit • No role for NSAIDs • Reliable results with surgical release • Occupational Therapy: Good evidence for relief of mild CTS symptoms with use of wrist brace at night. 4
9/26/2016 TRIGGER DIGITS • Mechanical catching of the digit during active extension and flexion • “Feels like my finger/thumb is coming out of joint” • “My finger gets stuck” • Morning locking/stiffness that improves as day progresses (similar to OA) TRIGGER DIGITS • Ring finger and thumb most common • Association with flexor tendon sheath cysts in palm • Can be association with carpal tunnel syndrome • Etiology • Idiopathic • Inflammatory • Trauma • Congenital 5
9/26/2016 TRIGGER FINGERS • ASSOCIATED RISK FACTORS • Diabetes Mellitus • Gender • Age • Previous history of trigger digits, CTS • Rheumatoid Arthritis • Occupation? TRIGGER DIGITS • EXAMINATION • Obvious mechanical triggering • Tender at palmar base of finger (A-1 pulley) • Can present with locked digit • Mild flexion contractures in chronic cases • Mobile “nodule” at A-1 pulley with finger motion • No X-Rays needed • Don’t confuse with Dupuytren’s or OA TRIGGER DIGITS • TREATMENT • Observation, rest • No role for NSAIDs other than pain relief • Corticosteroid injection into tendon sheath • Reliable surgical release • Role of Occupational Therapy, splinting 6
9/26/2016 DE QUERVAIN’S SYNDROME • More common in female population • Associated with breast feeding hand position “Mommy thumb” • Pain at the radial side of the wrist • Aggravated by thumb/wrist combined motion • Paresthesias in Sensory Branch Radial Nerve in chronic cases 7
9/26/2016 DE QUERVAIN’ SYNDROME • Tenderness at first dorsal compartment • Radiating pain with Finkelstein’s test • Swelling at first dorsal compartment • Occasional cyst from leading edge of FDC • Tinel’s over Sensory Branch Radial Nerve • Basal joint is nearby so check grind test • Wrist radiographs to assess for arthritis FINKLESTEIN’S TEST DE QUERVAIN’ SYNDROME TREATMENT • Bracing for symptomatic relief – Thumb Spica • Acetaminophen and/or NSAIDs for symptomatic relief • Corticosteroid injections • Role of Occupational Therapy – may be helpful AFTER injection • Surgical release is reliable 8
9/26/2016 DEQUERVAIN’S INJECTION BASAL JOINT ARTHRITIS • Gender (F:M 6:1) • Armstrong 1994, Xu 1998 • Age, 1/3 females over 50 yo • Etiology -Degenerative arthritis • Role of joint laxity • Kirk 1967, Eaton 1984, Pellegrini 1996 -Inflammatory arthritis –RA, psoriatic -Post-traumatic arthritis 9
9/26/2016 BASAL JOINT ARTHRITIS • ain and/or weakness with pinch and grip activities • CMC joint tender to palpation • Dorsal first CMC joint prominent with subluxation • Thumb in palm contracture, MCP hyperextension • Positive grind test • Confirmatory X-Rays • De Quervain’s can mimic basal joint OA, check Finklestein’s test BASAL JOINT ARTHRITIS TREATMENT • Rest • Bracing • Custom rigid thermoplastic orthoses • Soft supports • Nutritional supplements • Acetaminophen and/or NSAIDs • Corticosteroid injection • Role of Occupational Therapy – Hot Paraffin Dips, Bracing and Adaptive Equipment • Several reliable surgical options once conservative measures fail, dependent upon the stage of arthritis 10
9/26/2016 LATERAL EPICONDYLOSIS • Lateral Elbow pain • Weakness in grip • Symptoms aggravated by activities that involve resisted wrist and elbow extension • Insidious onset most common, but can be attributed to an event or activity 11
9/26/2016 LATERAL EPICONDYLOSIS • PHYSICAL EXAMINATION • Tenderness • Provocative Maneuvers • STUDIES • Plain films only if elbow motion reduced • Pomerance 2002 • Resist the urge to order MRI • Incidental extensor changes occur with age with high false positive rate • Steinborn 1999, LATERAL EPICONDYLOSIS EXAM LATERAL EPICONDYLOSIS • Histologic findings lead to the concept that this is a degenerative rather than inflammatory process – cortisone injections will likely not work in chronic cases. • This is an “OSIS,” NOT an “ITIS” 12
9/26/2016 TRADITIONAL TREATMENT • Rest/Ice • NSAIDs • Modification of activities • Elbow strap/wrist brace • Corticoid steroid injections • Occupational therapy - bracing and modified activities • Surgery for refractory cases CORTICOSTEROID INJECTION • Most effective early in process (first three months) in conjunction with occupational therapy • Consent to include possibility of: • Recurrence • Permanently altered skin pigmentation • Subcutaneous fat atrophy • Steroid flare 13
9/26/2016 LATERAL EPICONDYLOSIS WHAT WE DO KNOW • Enthesopathy of middle age • Unknown pain generator • No single reliable treatment • Surgical results inconsistent • Self limited condition, although it can last greater than 12 months. LATERAL EPICONDYLOSIS • Shared decision making with patient for treatment • Reassurance • Nothing is being damanaged • PAIN ≠ HARM • Improving coping strategies • Multidisciplinary effort LATERAL EPICONDYLOSIS: BRACES Use of Braces = Inconclusive • Wrist brace: • Consider trial of wrist brace at night if awakening with pain. • May also be helpful with heavy lifting. • Counterforce brace: • Caution: compression can irritate radial and ulnar nerves. • Wear with activity and use model with built-in pad. 14
9/26/2016 CUBITAL TUNNEL SYNDROME • Second most common peripheral compression (entrapment) neuropathy • Prevalence 2-3 % of adults • Equal male/female involvement • Etiology • Idiopathic • Traction • Compression CUBITAL TUNNEL SYNDROME • Associated risk factors • Diabetes Mellitus • Previous h/o elbow fracture • Nerve Subluxation • Elbow arthritis/synovitis CUBITAL TUNNEL SYNDROME • Paresthesias (pins & needles) in the ulnar nerve distribution including ulnar aspect of hand • Weak grip • Weak pinch • Loss of dexterity “my hand does not do what I tell it to do” 15
9/26/2016 CUBITAL TUNNEL SYNDROME Examination • Ulnar nerve tinel’s at elbow • Altered sensation by monofilament testing • Positive elbow flexion test • Weak inter-osseous musculature • Flexible ulnar clawing, Wartenburg’s T sign, Froment’s sign • Wasting of hand intrinsics • Confirmatory NCS “IR NCS” • X-Rays of the elbow CUBITAL TUNNEL SYNDROME • Treatment • Avoiding aggravating activities and positions • Prolonged elbow flexion • Direct pressure on medial elbow • Corticosteroid injections are discouraged – due to risk of nerve injury • Surgery in recalcitrant cases • Role of Occupational Therapy – night bracing 16
9/26/2016 DUPUYTREN’S DISEASE (PALMAR FIBROMATOSIS) • Typically painless other than onset • Sub-Q nodule in palm of hand at distal palmar crease (level in line with ring/little metacarpal) • Over time form pretendinous cords • +/- Contracture of MCP joint • +/- Extension into digit & PIP joint contracture • Knuckle pads at MCP/PIP joints PALMAR FASCIA Dupuytren’s Disease 17
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries