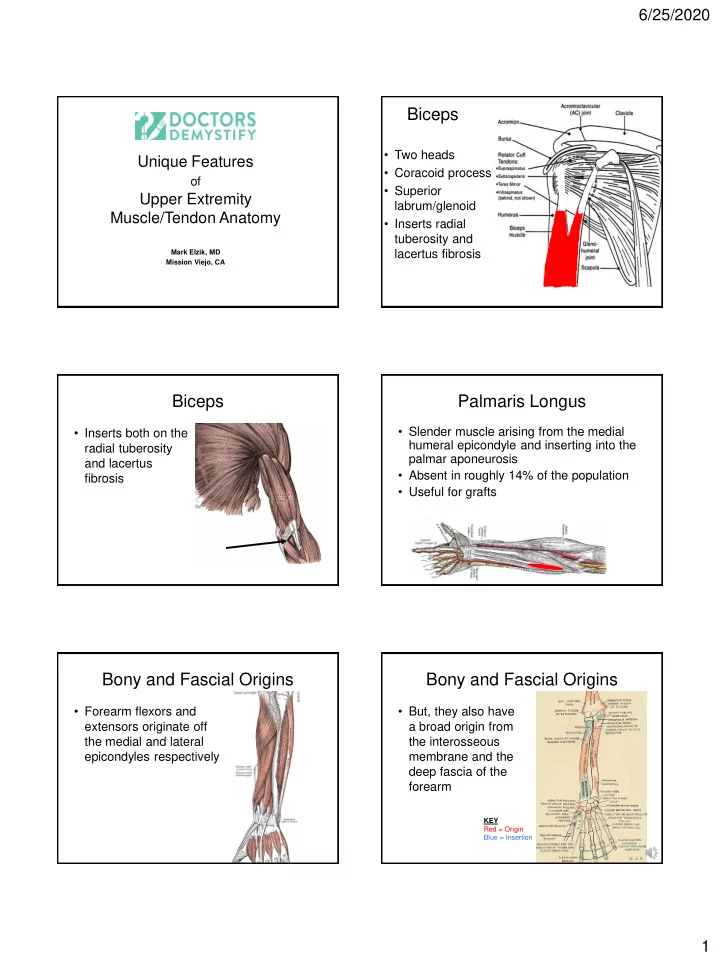
6/25/2020 Biceps • Two heads Unique Features • Coracoid process of • Superior Upper Extremity labrum/glenoid Muscle/Tendon Anatomy • Inserts radial tuberosity and Mark Elzik, MD lacertus fibrosis Mission Viejo, CA Biceps Palmaris Longus • Slender muscle arising from the medial • Inserts both on the humeral epicondyle and inserting into the radial tuberosity palmar aponeurosis and lacertus • Absent in roughly 14% of the population fibrosis • Useful for grafts Bony and Fascial Origins Bony and Fascial Origins • Forearm flexors and • But, they also have extensors originate off a broad origin from the medial and lateral the interosseous epicondyles respectively membrane and the deep fascia of the forearm KEY Red = Origin Blue = Insertion 1
6/25/2020 Bony and Fascial Origins Lumbricals • Origin – FDP • These broad muscular origins allow tendon the muscle to maintain resting length • Insertion – and function when their bony Extensor Expansion attachments are released • Fascinating – Medial epicondylectomy for cubital muscle as it has tunnel NO bony origin – Lateral release for tennis elbow or insertion Interosseous Muscles (Palmar) Interosseous Muscles (Dorsal) • 4 dorsal interosseous • 3 palmar muscles interosseous muscles • Originate from • Originate from metacarpals & insert metacarpals & insert onto proximal phalanx onto proximal phalanx bases/extensor bases expansion • Responsible for • Responsible for adduction of the fingers aka “ PAD ” abduction of the fingers aka “DAB” Camper’s Chiasm Annular (A) pulleys generally located mid-bone and do the heavy lifting • FDS begins superficial/volar to FDP Cruciate (C) pulleys generally over the joints and • FDS splits just proximal to the PIP, rotates can collapse during digital flexion 180 degrees and inserts on the MP deep Proximal Middle Distal phalanx phalanx phalanx to the FDP Collateral ligament FDP tendon Horst: Training for Climbing 2
6/25/2020 References thanks for listening • Gray H. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918. • Susman RS, Nyati L, Jassal M. Observations on the Pollical Palmar surgeons providing excellence in education Interosseous Muscle (of Henle). Anat Rec for OTs and PTs since 1990 1999;254:159 – 165. • Snell RS. Clinical Anatomy 6 th Ed. 2000. • Tan ST, Smith PJ. Anomalous Extensor bibliography on following slides Muscles of the Hand: A Review. J Hand Surg 1999; 24A:449 – 455. Muscle Physiology and Mechanics Muscle Physiology • Muscle Fibers - Types and Conditioning and Mechanics • Physiology of Muscle Contraction Stewart Brown, M.D. • Basic Biomechanics of Joint Motion Fast Twitch Muscle Fibers Slow Twitch Muscles Fibers • Distance runners • Sprinters – Aerobic – Anaerobic – Contraction – slow – Contraction - fast – Fatigue resistance – high – Fatigue resistance – low 3
6/25/2020 Muscle Strengthening Blood Flow Restriction BFR Muscle cell hypertrophy = Protein synthesis • 60% arterial occlusion – Diet pressure gives maximum effect – Exercise – Hormones • Lower cuff pressure is less painful Muscle Atrophy Blood Flow Restriction BFR Trauma, Immobilization, Nerve injury, … • 40% 1Repetition Protein synthesis maximum instead of 70% effective Number of muscle • 2 Cochrane nuclei normal registered Patterson et al , Blood Flow prospective Restriction Exercise: Recovery Potential Considerations of Methodology, studies ongoing Thenar Atrophy in Carpal Application, and Safety Good Tunnel Syndrome https://www.frontiersin.org/article/10 .3389/fphys.2019.00533 Muscle Ischemia Skeletal Muscle Loss of perfusion of the muscle Cell death Striated Muscle Fibrous scar Multinucleated cells Recovery Potential Myofibrils Muscle necrosis after Myosin dark bands Compartment syndrome Actin light bands 4
6/25/2020 Striated Muscle Contraction Striated Muscle Relaxation Ca ++ C a ++ Actin Actin Actin Actin Myosin Myosin Maximum tension is proportional to the Arrangements of muscle’s cross -section Sarcomeres parallel adm series lumbrical Which arrangement of sarcomeres has a stronger excursion? Which has a longer excursion? Active Active • Strongest at resting length Contraction Muscle produces its highest Contraction (greatest actin-myosin contact) tension (strongest contraction) at its resting length Tension (stress) It produces less tension Tension when it is shorter or longer. Length Length (strain) 5
6/25/2020 Moment Arm Equals the perpendicular distance between the joint’s center of rotation and the crossing Who is the Jamar set up tendon for? What’s happening here? Reading Quiz! Brand P, Hollister, A: Clinical Mechanics of the Hand . Ed. 3, St. Louis, Mosby, 1999 Gonzalez et al. Biomechanics of the Digit. JASSH , 2005. Little J, Phillips S:Resistance exercise and nutrition to counteract muscle wasting.Appl Physiol Nutr Metab. 2009 34:817-28 A2 pulley rupture. Rassier: Molecular basis of force development by How does this affect the function skeletal muscles during and after stretch. Mol Cell Biomech. 2009 6:229-41. of the finger? Escamilla R, et al: Shoulder muscle activity and function in common shoulder rehabilitation exercises. Sports Med. 2009;39:663-85 Tendon Biology Surgeons providing excellence in education for OTs and PTs since 1990 pro Paul Garheeb, MD 6
6/25/2020 Tendon Healing Tendon Vascularity • Tendons appear inert but nutritional pathways • Vincula supply must be maintained or restored for healing to capillaries to occur • Tendon capillaries come from dorsal 2/3 of – musculotendinous junction flexor tendons – bone insertion within digital – vincula • Synovial fluid nutrition occurs within the tendon sheath sheath – volar and dorsal wrist – digital flexor tendon sheath avascular zone volarly Tendon Vascularity avascular zones Tendon Vascularity • Significant areas of • Blood supply to zone 2 tendons have no blood supply and tendon leaves fds rely on synovial avascular zones diffusion for between vincula nutrition fdp Intrinsic/Extrinsic Tendon Healing Intrinsic/ExtrinsicTendon Healing • Intrinsic healing: tenocytes within • Extrinsic healing: tendon can heal injury without tendons do not have granulation from surrounding tissues capacity for self- healing, rely on granulation tissue from surrounding areas to invade injury site 7
6/25/2020 Phases of Wound Healing Tendon Healing • Experimentally, tendons can clearly II. inflammation III. proliferation IV. maturation I. hemostasis heal by intrinsic means collagen • Clinically, tendons likely heal by accumulation combination of intrinsic and extrinsic means 0 3 10 30 100 300 days Prevention of Adhesions The Dream The Facts Goal of Tendon Healing • Mechanical barriers *Ineffective - Artificial materials *Obstructive • To allow tendon healing while avoiding - Sheath closure tendon-sheath adhesions – strong suture, strong technique, strong knot • Pharmacological agents – minimal interference of vascularity - Anti-inflammatories - Chemical barriers *Nonselective - Collagen degraders Prevention of Adhesions--The Reality Tendon Gliding sheath early tendon scar motion bone • Accelerates development of tensile 1 wound, 1 scar. 1 wound, 2-3 scars strength • Reduces restrictive adhesions • Forces must be kept below level of suture disruption immobilized tendon repair mobilized tendon repair 8
6/25/2020 How many medium sized apples in a How much force is generated pound? in a tendon? Fact: ~5 apples in a pound • Passive finger motion generates 9 Newtons • Active unresisted flexion generates 35 N Fact: ~5 Newtons in a pound • 8 pounds of pinch (40 N) generates 120 N 1 N = Most repair techniques withstand 20-30 N What is a Newton? (Not a fig newton) 1 N ~ .2 pound Tendon Grafting A Multitude of Tendon Repair Techniques Conventional donor sites extrasynovial tendons • Suture selection: palmaris longus • Size: 3-0 vs 4-0 plantaris (adjacent to Achilles tendon • Type: braided vs. monofilament Experimental donor sites • Material: nylon vs. many others intrasynovial tendons FDP, FDS in zone 2 • Suture technique: 2-strand vs. 4, 6, 8-strand digital flexors/extensors under wrist retinacula • Tendon grasping maneuvers Tendon Grafting rough surface of Tendon Healing: Key Points grafted • Tendons have low metabolic demands • Intrasynovial donor extrasynovial • Tendons have low metabolic supply tendons (experimental) donor tendon – fewer adhesions (more • Tendons generally heal by combination of intrinsic healing) intrinsic/extrinsic healing – less friction around • Differential gliding of tissues only current annular ligaments way to modulate adhesion formation – result: less force • Ask surgeon how strong the repair is during required to achieve smooth surface of early therapy gliding grafted intrasynovial donor tendon 9
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries