TELEHEALTH - Innovation in Healthcare Delivery Midland Region joint Boards, 7 November 2014 Simon Everitt, BOP GM Planning and Funding, Owen Wallace, BOP GM Information Management Ernie Newman, Project Coordinator 1
Agenda • Introduction to Telehealth • What is Telehealth? • What is the existing base? • Creating a Telehealth Community • Demonstration Project • Observations / Lessons Learned • Opportunities for Future • Making it sustainable • Regional Perspective 2
What Is Telehealth? • Means many things! Examples: 1 Use of telecommunications as an enabler of clinical or managerial communication involving health services 2 Video consultations in which there is a patient present, and remote monitoring of patients’ conditions • “Telehealth” is understood in the sector, but for public understanding we are learning to talk about “Video Doctor services” or “Video Outreach Clinics.” • Today in the context of the BoP and the Project we are focused on the use of video communication for clinical consultations between health professionals and patients. 3
NZ Telehealth Examples • NZ Telepaediatrics – national network delivering Starship grand rounds & clinician support (10+yrs) • Canterbury / West Coast – remote support for primary and secondary service delivery in West Coast (10+yrs) • Waikato – Teledermatology service (10+yrs) • Northland – base hospital support for rural facilities eg Renal service between Whangarei & Kaitaia (5yrs) • BOP – Mental Health clinical support service (5+yrs) • Te Whiringa Ora – community based remote monitoring (3yrs) • Regional Cancer Networks – Multi Disciplinary Meetings support (<2yrs)
Telehealth Demonstration Project • Ministry of Business, Innovation and Employment • Wanted to explore how Ultra Fast Broadband and Rural Broadband would be used in health • National Health IT Board • Telehealth is part of the Health IT Plan, wanted to learn more of what works and otherwise in NZ setting • Bay of Plenty District Health Board • Selected for the Project because of existing commitment • Tairawhiti District Health • Joined early 2014 – significant potential benefits 5
The 2 Phases Of The Project: March 2013 - August 2014 – “Evangelise and Scatter” – supply cameras and connectivity to suitable health sites with receptive professionals, encourage use, and learn from the results. September 2014 - February 2015 – “Consolidate and Sustain” – build usage and scale into established video infrastructure, aiming for regular usage within solid, sustainable frameworks. 6
Telehealth Project “Community”
Map dated Nov 2013. Since added Te Araroa, Tikitiki, Ruatoria,Te Puia, Tokomaru Bay, Tolaga Bay, Gisborne x5, Kawerau, Katikati, Te Puna VIDEO CAPABILITY SEPT 2014
3 Examples of Telehealth Service: • Video Outreach Clinics • Video Doctor Services • Emergency Support 9
VIDEO OUTREACH CLINIC Church Street Surgery, Opotiki
Video Outreach Clinics: • Hospital-based services being delivered to patients in outlying communities – Examples: • Diabetes, Tauranga hospital to Opotiki practice – operating • Diabetes, Gisborne Hospital to Te Puia and Tokomaru Bay Hauora – starting early November • Mental Health Christchurch specialist with Tauranga patients, and Gisborne hospital with Ngati Porou clinics - operating • Renal, Hamilton Hospital to Whakatane Hospital – starting 18 November 11
Video Doctor Service: GPs consulting patients in hard-to-reach communities by video. Examples: • Te Awanui Hauora on Matakana Island, with Te Akau Hauora at Papamoa Beach – operating; to be joined by Katikati and Te Puna • Ngati Porou sites – patient at one clinic with GP at another – coming soon • Video:
EMERGENCY SUPPORT Treatment room, Opotiki Community Health Centre
Emergency Support • Video support for front line staff handling emergency situations • Examples: • Opotiki Community Health Centre - Video support from duty GP at home after hours • Whakatane-Tauranga ED/ICU support (pre-dated Project) – limited usage • Gisborne Hospital support for Ngati Porou clinics in emergency – yet to convince Gisborne ED doctors 15
Other Opportunities Awaiting: The opportunity: 16
Opportunities: • Smoking cessation – already trialed Gisborne-Ruatoria • Palliative care (3 hospices video-enabled) • Mental health – child and adolescent, addiction services • Chronic Conditions - Cardiology, Respiratory (COPD)? • Maternity – eg Rural birthing units to O&G support? • Allied Health - eg Dietitian? • Other? 17
The Payback: Major Beneficiaries • Short Term – • Patients in isolated communities, • Health professionals - reduced need to travel / more consult time, support for rural practitioners • Medium term – • Chronic condition patients - comprehensive, timely and less intrusive management via combination of video and remote monitoring; • Health professionals working to full extent of their practice capabilities • Long term – • Patients who currently miss out on treatment will be captured and treated earlier due to easier interaction with services, with a wide range of savings from earlier intervention 18
The Potential Is Enormous: • Earlier interventions & better deployment of clinical resources • Lower travel time & $ for patients - timely treatment, reduced DNAs • Earlier intervention - longer term cost savings • Reduced locum & travel costs for DHB A key enabler of 21 st century health service delivery systems, • designed to cope with aging population, aging health workforce, and advanced health technologies • Telehealth does not exist in isolation. It enables change but does not itself create change. Requires re-engineering of services if telehealth isn’t to become expensive overhead. 19
Observations & Lessons Learned
“Telehealth Is Easy” Because: • Technology & connectivity aren’t the issue: • Entry level technology is inexpensive to install • Connectivity has improved markedly in recent years • The running cost is low – a video call within NZ is often cheaper than an equivalent voice toll call • Client adoption - many users understand and are comfortable with video due to early, “free” examples such as Skype 21
“Telehealth Is Hard” Because: • Telehealth is disruptive to conventional ways of working: • impact on clinical work flows • remuneration structures / practices • medico-legal accountabilities and risk • how disparate groups work together – primary/secondary/tertiary; doctor/nurse; hospital clinics • Video challenges the basic tenet that the only way for a patient to consult a clinician is one-on-one, face-to-face • Network carrier commercial arrangements and behaviours inhibit widespread expansion 22
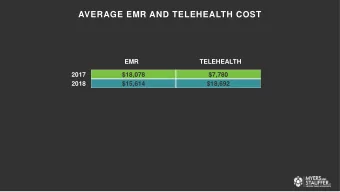
Lessons • It only takes a handful of visionaries to start a movement for change; the trick is to identify and work with them • Speed of adoption - Primary / Community vs Secondary • Sustaining the gains requires stakeholder commitment and leadership • Challenge of appropriate investment: • End Points: $300 to >$30,000 • Rooms: <$5000 to >$60,000
Where To From Here? • Regional Telehealth Strategy - developed 2013/14 • Regional Telehealth Advisory Group – transition from interest group to advisory group Chaired by Dr Ruth Large, Waikato ED specialist • Regional Co-ordination – development of consistent approaches - policy, protocol, standards, templates • Local operational delivery – engagement and adoption likely to be greatest at local &/or sub-regional levels 24
Questions / Discussion
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries