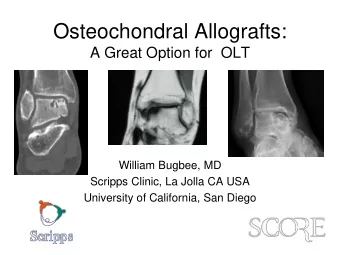
Osteochondral Allografting of the Knee William Bugbee, MD Director, Cartilage Transplantation Program Scripps Clinic, La Jolla CA Professor, University of California, San Diego
Disclosure • Joint Restoration Foundation – Consultant, research support • Arthrex – consultant • FDA – Medical advisory committee: Cellular, tissue and gene therapy
Fundamental Strategies of Cartilage Restoration • Cell based – Induce cells to form (chondral) tissue in situ – Marrow stimulation – ACI – Other cell sources • Whole tissue based – Restore defect with mature tissue – Osteochondral autograft (OAT) – Osteochondral allograft (OCA) – Processed (acellular) allografts
“Seed vs. Sod”
Subchondral Bone and the Osteochondral Unit • Integrated organ system • Interdependent structure- function relationship
Cartilage is an Ideal Tissue for Transplantation • Avascular • Aneural • Immunoprivileged • Amenable to storage • Can be fashioned to fit recipient
Advantages of Osteochondral Repair • Mature hyaline cartilage • Bone healing paradigm • Replace diseased subchondral bone • Faster and simpler rehabilitation
Nomenclature for Osteochondral Grafts • Osteochondral autograft transfer • Osteochondral allograft = OAT transplant = OCA • Mosaicplasty = transfer of more • Allograft OATS = ? than one plug • Fresh = never frozen • OATS = trademarked name of • Stored/refrigerated surgical instrument set • Fresh-frozen (?) • Frozen
Osteochondral Allograft Transplantation • Originally introduced as a joint reconstructive procedure for trauma, tumor reconstruction • Now widely used as a cartilage restoration technique for chondral and osteochondral lesions • San Diego program began in 1983 Cartilage repair paradigm Complex reconstruction paradigm • Microfracture • OCD • OAT • AVN • ACI • Post-traumatic • OCA
Governing Principles for Fresh Allograft Use Cartilage Repair • Whole tissue transplant • Viable chondrocytes in mature hyaline cartilage matrix • No cell or tissue differentiation required • Maximizing and preserving inherent chondrocyte and matrix properties critical • Cells within matrix are Immunoprivileged • Allograft chondrocytes survive transplantation and maintain matrix
Governing Principles for Fresh Allograft Use in Cartilage Repair • Osseous portion is a nonliving scaffold and interface for attachment and integration • Minimal volume unless osseous reconstruction necessary • Incorporation by creeping substitution • Potential site for immunologic response by recipient • Behavior of osseous component is important predictor of clinical success
Indications for Osteochondral Allografts • Osteochondritis dissecans/OLT • Traumatic chondral/osteochondral lesions • Revision of previous cartilage surgery • Osteonecrosis/ SONK • Fracture malunion (tibial plateau) • Focal degenerative chondral lesions • Osteoarthritis
Surgical Techniques • Dowel or plug Focal lesions • – 10-30 mm – Femoral condyle, trochlea, patella, humeral head, femoral head • Shell graft – Complex, inaccessible lesions – Femoral condyle, trochlea, tibia, talus • Small fragment – Large or deep lesions – Tibia, patella, glenoid
Surgical Technique: Femoral Condyle
Surgical Technique: Femoral Condyle
Large Lesions: Multiple Grafts
Multiple Grafts
Patellar Allograft
Tibial Plateau and Meniscus
Allografting of Other Joints • Ankle – OLT – Osteoarthritis – AVN • Shoulder – AVN – Chondral or osteochondral lesions • Hip – AVN – Trauma • Small joints
Femoral Head Allograft
Humeral Head Allografting
Clinical Outcomes by Diagnosis Among patients with grafts in situ at latest follow-up Mean Mean OCA IKDC IKDC Diagnosis failure pain Function Satisfaction* Traumatic chondral injury 2% 3.3 7.3 90% Osteochondritis dissecans 7% 2.1 8.1 96% Fracture 15% 4.4 6.1 80% Degenerative chondral lesion 21% 3.7 6.3 81% Avascular necrosis 25% 2.7 7.1 92% Osteoarthritis 39% 3.5 5.8 79% *responded either “satisfied” or “extremely satisfied”
Clinical Outcome
Patient Satisfaction at Latest Follow-up 89% satisfied 100% 100% 80% 80% 68% 68% 60% 60% 40% 40% 21% 21% 20% 20% 6% 6% 3% 3% 2% 2% 0% 0% Extremely Extremely Satisfied Satisfied Somewhat Somewhat Somewhat Somewhat Dissatisfied Dissatisfied satisfied satisfied satisfied satisfied dissatisfied dissatisfied
Postoperative Rehabilitation • Depends on graft size, fixation and location • Concurrent procedures such as ACL, osteotomy, meniscal repair or transplantation generally guide Rx • Simple outline – Protect weight bearing (25%) for 4-6 weeks – No ROM restrictions except occasionally for PF grafts – No routine bracing or CPM – Rule of thumb: treat like a fracture that has been fixed • Clear advantage of OCA: simple and rapid rehabilitation in spite of need for arthrotomy
Rapid recovery after OCA • Tissue maturation not required – Best quality at time=0 – No ROM restrictions • Excellent initial graft stability • Bone healing occurs rapidly – 4-6 weeks – Protected wt bearing 0-4 weeks • Functional recovery – Arthrotomy – Neuromuscular – Between 3-6 months
Return to Sports After OCA Unable to perform any activities 1.8% Fair function Did not return Light 10.3% to sports activities Excellent Good 24.8% 19.7% function function Very strenuous 36.7% 18.6% activities 37.2% Moderate Returned to activities Very good function sports 75.2% 25.0% Strenuous 34.4% activities 16.3% 78.5% 75.2% 71.1% able to participate in very good to returned to high lev&77el of excellent function sport activity
Variables predicting return to sport •Males more likely than females Gender p=0.042 •to return to sport •Patients sustaining a sports-related injury more Etiology of injury p=0.005 likely to return to sport •Patients with osteochondritis dissecans more Diagnosis p=0.001 likely to return to sport than those with a degenerative chondral lesion Anatomical •Patients with unifocal condylar lesions more p=0.004 likely to return to sport than multifocal or location of graft patellar lesions •Patients with smaller grafts more likely Graft size p=0.042 •to return to sport Patient age and duration of symptoms not significant
25% did not return to sport….why? 0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50% Pain 47% Worried about re-injury 41% Clicking or grinding 41% Stiffness 35% Could not fully bend 29% Other problem with knee 25% Knee-related problems Instability 18% Instructed not to participate 12%
25% did not return to sport….why? 0% 5% 10% 15% 20% 25% Health issues unrelated to knee 24% Less interest in sports 12% Started a family Lifestyle 6% reasons Changed jobs or career 6%
Osteochondral Allografts in 2017 • A mainstream treatment option (more OCA than ACI performed in US) • Proven safety, efficacy and versatility • Addresses the common subchondral bone disease • High rate of return to ADLs, sports and recreation • High acceptance and patient satisfaction
Thank You
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries