OPTICS in Cardiology Zürich, April 20./21., 2018 New LDL lowering drugs - How to select the patients? Wolfgang Koenig, MD, FRCP, FACC, FAHA, FESC Professor of Medicine/Cardiology Klinik für Herz - & Kreislauferkrankungen Deutsches Herzzentrum München Technische Universität München
Conflict of Interest (COI) - Disclosure Honorarium for Lectures: AstraZeneca, Novartis, MSD, Amgen, Sanofi, Actavis, Berlin-Chemie Consulting : Novartis, Pfizer, The Medicines Company, Amgen, AstraZeneca, MSD, Kowa Participation in Clinical Trials : LEADER (Novo Nordisk), CANTOS (Novartis), FOURIER, GLAGOV (Amgen), OPTIONS I und II (Sanofi/Regeneron), SPIRE (Pfizer), CAIN III (MHICC), PROMINENT (Kowa), DalGene (DalCor), COLCOT (MHICC) Research Contracts: Abbott, Roche Diagnostics, Beckmann, Singulex Stockholder of a Healthcare Company: none
Preferred Pharmacotherapy Formulary High-intensity Statin Therapy (>50% LDL-C reduction) Initial drug monotherapy Rosuvastatin or atorvastatin If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to two-drug combination Two-drug Combination Three-drug Combination Complex-therapy Combination Gidding et al. Circulation 2015;132
Preferred Pharmacotherapy Formulary High-intensity Statin Therapy (>50% LDL-C reduction) Initial drug monotherapy Rosuvastatin or atorvastatin If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to two-drug combination Two-drug Combination Rosuvastatin or Atorvastatin + Ezetimibe If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to three-drug combination Three-drug Combination Complex-therapy Combination Gidding et al. Circulation 2015;132
Preferred Pharmacotherapy Formulary High-intensity Statin Therapy (>50% LDL-C reduction) Initial drug monotherapy Rosuvastatin or atorvastatin If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to two-drug combination Two-drug Combination Rosuvastatin or Atorvastatin + Ezetimibe If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to three-drug combination Three-drug Combination Rosuvastatin or Atorvastatin Rosuvastatin or Atorvastatin Rosuvastatin or Atorvastatin + + + Ezetimibe Ezetimibe Ezetimibe + + + Colesevelam or other Niacin PCSK9 inhibitors bile acid sequestrant If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to complex-therapy combination Complex-therapy Combination Gidding et al. Circulation 2015;132
Preferred Pharmacotherapy Formulary High-intensity Statin Therapy (>50% LDL-C reduction) Initial drug monotherapy Rosuvastatin or atorvastatin If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to two-drug combination Two-drug Combination Rosuvastatin or Atorvastatin + Ezetimibe If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to three-drug combination Three-drug Combination Rosuvastatin or Atorvastatin Rosuvastatin or Atorvastatin Rosuvastatin or Atorvastatin + + + Ezetimibe Ezetimibe Ezetimibe + + + Colesevelam or other Niacin PCSK9 inhibitors bile acid sequestrant If LDL-C above goal after 3 months of therapy and patient is adherent, proceed to complex-therapy combination Complex-therapy Combination Consider four-drug combination and LDL Apheresis Gidding et al. Circulation 2015;132
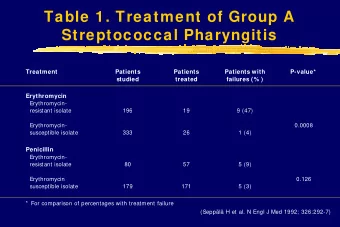
High Risk Patients Achievining a LDL-C <70 mg/dL, stratified by Baseline LDL-C ≥160 mg/ dL Unmet Medical Need: Familial Hypercholesterolemie (he/ho) Patients with statin intolerance High risk patients with progressive atherosclerosis manifestations who do not Dose (mg) achieve a LDL-C goal <70 mg/dL Atorvastatin Simvastatin Rosuvastatin Based on those studies providing direct comparisons for patients with baseline LDL- C ≥160 mg/ dL, rosuvastatin 10 – 40 mg doses were significantly superior to equal and double doses of atorvastatin and simvastatin (p<0.01) Note: p values for rosuvastatin vs Nicholls SJ et al. Am J Cardiol 2010; 105: 69 – 76 simvastatin are data on file, AstraZeneca Lundman P et al. Atheroscler Suppl 2011; 12: 164 (abstract) Adapted by permission from Elsevier Inc.
Hepatic LDL-Rs Play a Key Role in the Regulation of Plasma LDL-C Concentrations LDL 1. Brown MS, Goldstein JL. Proc Natl Acad Sci U S A. 1979;76:3330-3337. 2. Steinberg D, Witztum JL. Proc Natl Acad Sci U S A. 2009;106:9546-9547. 3. Goldstein JL, Brown MS. Arterioscler Thromb Vasc Biol. 2009;29:431-438.
PCSK9 Regulates the Expression of Hepatic LDL-Rs on the Cell Surface 1. Qian YW, Schmidt RJ, Zhang Y, et al. J Lipid Res. 2007;48:1488-1498. 2. Horton JD, Cohen JC, Hobbs HH. J Lipid Res. 2009;50(suppl):S172-S177
Anti-PCSK9 Monoclonal Antibodies Block the PCSK9/LDL-R Interaction and Lower LDL-C 1. Chan JC, Piper DE, Cao Q, et al. Proc Natl Acad Sci U S A. 2009;106:9820-9825.
Proprotein Convertase Subtilisin/kexin 9: PCSK9 Inhibitors Lower LDL-C by 50-60% independent of the patient`s background risk and the lipid lowering regime Long-term efficacy with 2 or 4-weekly injections (DESCARTES, FOURIER, ODYSSEY) LDL-C goal (<70 mg/dL) achieved in 70-90% of patients Lowering of Lp(a) by appr. 30% So far excellent tolerability and safety
FOURIER Study Design Sabatine MS et al. Am Heart J 2016;173:94-101
Summary of Effects of the PSK9 Inhibitor Evolocumab LDL-C by 59% down to a median of 30 mg/dl • First CV endpoint trial in patients on statin therapy • • Safe and well-tolerated (42% of patients had a LDL-C < 25 mg/dl) HR 0.85 (0.79-0.92) Placebo P<0.0001 No reduction of cardiovascular death • HR 0.80 (0.73-0.88) 59% reduction Clinical benefit driven by a reduction of MI, stroke • P<0.0001 P<0.00001 and coronary revascularisation Absolute 56 mg/dl Efficacy increases with extended FU (Landmark • Analysis) Evolocumab (median 30 mg/dl, IQR 19-46 mg/dl) CVD, MI, stroke CVD, MI, stroke UA, cor revasc Sabatine MS et al. NEJM 2017;376:1713-22
Primary and Secondary Endpoint in Patients With and Without PAD Bonaca et al. Circulation 2018;137:338-350
MACE or MALE in Patients With and Without PAD Bonaca et al. Circulation 2018;137:338-350 MACE: MI, stroke, CV death – MALE : acute ischemia, revasc. amputations
Benefit of Evolocumab Based on Time From Qualifying MI Sabatine et al Circulation 2018 (epub ahead of print)
Benefit of Evolocumab Based on Number of Prior MIs Sabatine et al Circulation 2018 (epub ahead of print)
Benefit of Evolocumab Based on Multivessel Disease Sabatine et al Circulation 2018 (epub ahead of print)
ODYSSEY: Study Design Randomized 18,924 patients Alirocumab Placebo (N=9462) (N=9462) Follow-up*: median 2.8 (Q1 – Q3 2.3 – 3.4) years 8242 (44%) patients with potential follow-up ≥ 3 years • Premature treatment 1955 patients experienced a primary discontinuation endpoint 726 patients died • Blinded switch to placebo (2 consecutive LDL-C values <15 mg/dL) 1343 (14.2%) 1496 (15.8%) • Patients lost to follow-up (vital 730 (7.7%) Not applicable status) 14 9 *Ascertainment was complete for 99.1% and 99.8% of potential patient-years of follow-up for the primary endpoint and all-cause death, respectively Steg et al ACC 2018
ODYSSEY: Primary Endpoint ARR* 1.6% HR 0.85 MACE: CHD death, (95% CI 0.78, 0.93) non-fatal MI, ischemic P=0.0003 stroke, or unstable Steg et al ACC 2018 angina requiring hospitalization *Based on cumulative incidence
ODYSSEY: Prespecified Subgroups Incidence (%) Subgroup Patients Alirocumab Placebo HR (95% CI) p-value* *P-values for interaction 20 20 20 100 mg/dL 80 to <100 mg/dL <80 mg/dL 16 16 16 MACE (%) MACE (%) MACE (%) 12 12 12 Placebo 8 8 8 Alirocumab 4 4 4 0 0 0 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 Years Since Randomization Years Since Randomization Years Since Randomization Number at Risk Number at Risk Number at Risk Placebo 3583 3347 3122 1290 256 Placebo 3062 2889 2708 1195 195 Placebo 2815 2568 2371 986 178 Alirocumab 3581 3365 3183 1327 233 Alirocumab 3066 2880 2732 1194 213 Alirocumab 2814 2602 2431 1053 207
Algorithm for the Use of PCSK9 I in Patients With ASCVD and Substantially Elevetaed LDL-C Patients with clinical ASCVD (CAD, symptomatic PAD, ischaemic stroke) On maximally tolerated statin therapy ± Ezetimibe* *According to clinical judgement and local guidance LDL-C >3.6 mmol/L LDL-C >2.6 mmol/L (>100 mg/dL) and with additional indices of risk severity § (>140 mg/dl) § Including • Familial hypercholesterolaemia Consider a PCSK9 • Diabetes mellitus with target organ damage (e.g. proteinuria), inhibitor or with a major risk factor such as marked hypertension • Severe and/or extensive ASCV (e.g. severe polyvascular disease, extensive coronary disease – refer to Box 3) • Rapid progression of ASCVD, i.e. repeated ACS, unplanned coronary revascularization, or ischaemic strokes within 5 years Landmesser et al. of the index event EHJ 2017;0:1-13
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries