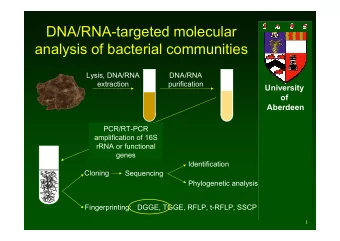
Extracorporeal support in critically ill Extracorporeal support in - PowerPoint PPT Presentation
Extracorporeal support in critically ill Extracorporeal support in critically ill patients : patients : When, How and How Much? When, How and How Much? Claudio Ronco, MD Claudio Ronco, MD Department of Nephrology, Department of Nephrology,
Extracorporeal support in critically ill Extracorporeal support in critically ill patients : patients : When, How and How Much? When, How and How Much? Claudio Ronco, MD Claudio Ronco, MD Department of Nephrology, Department of Nephrology, St. Bortolo Hospital, St. Bortolo Hospital, International Renal Research Institute International Renal Research Institute Vicenza Vicenza - - Italy Italy
1. Indications Indications 1. 2. Timing of initiation (+/ Timing of initiation (+/- - discontinuation) discontinuation) 2. 3. Modality Modality 3. 4. Dose/prescription Dose/prescription 4.
� Non Non- -obstructive oliguria ( obstructive oliguria (> >200mL/12 hr) or anuria 200mL/12 hr) or anuria � � Azotemia (urea Azotemia (urea>30 mmol/L) or uremic organ involvement >30 mmol/L) or uremic organ involvement � � Hyperkalemia (K+ >6.5 mmol/L) or rapidly rising Hyperkalemia (K+ >6.5 mmol/L) or rapidly rising � � Severe acidemia (pH <7.1) from metabolic acidosis Severe acidemia (pH <7.1) from metabolic acidosis � � Progressive and/or uncontrolled dysnatremia Progressive and/or uncontrolled dysnatremia � � Uncontrolled hyperthermia and/or hypothermia (>39.5 C) Uncontrolled hyperthermia and/or hypothermia (>39.5 C) � � Clinically significant, diuretic Clinically significant, diuretic- -unresponsive organ edema unresponsive organ edema � � Drug overdose with dialyzable toxin Drug overdose with dialyzable toxin � � Coagulopathy requiring large amount of blood products Coagulopathy requiring large amount of blood products � Any Critical Care or Nephrology Textbook
Renal Replacement Therapy Renal Support Therapy � Nutrition support Life Threatening � Absolute � Indications � Volume removal in refractory CHF � Immuno-modulation in sepsis � Solute control � Cancer chemotherapy � Fluid balance � Attenuate ARDS-induced respiratory � Acid-base regulation acidosis � Volume homeostasis in multi-organ dysfunction/failure Mehta CRRT 2008 Conference
Apache - - SOFA SOFA Apache 1 2 3 4 5 1 2 3 4 5 RRT RRT RRT RRT RRT RRT RRT RRT RRT RRT M O S T Score M O S T Score SCUF SCUF SCUF SCUF SCUF SCUF SCUF SCUF ECLS ECLS ECLS ECLS ECLS ECLS LiverS LiverS LiverS LiverS HVHF- HVHF -CPFA CPFA 100 100 Mortality % Mortality 80 80 60 60 40 40 % 20 20 0 0 K + 3 K + 3 Kidney K + 1 K + 2 K + 3 Kidney K + 1 K + 2 K + 3 + Sepsis + Sepsis
CRRT ECLS LiverSupport - HVHF SCUF CPFA - CAST
� Onset of symptoms? � Onset of symptoms? � Biochemical/biomarker thresholds? � Biochemical/biomarker thresholds? � Relative to onset of AKI? � Relative to onset of AKI? � Relative to ICU admission? � Relative to ICU admission? � RIFLE Class? � RIFLE Class? Numerous factors/complex process Numerous factors/complex process No broad consensus to guide No broad consensus to guide
� Considerable variation in RRT practice Considerable variation in RRT practice � � Surveys of Practice (Europe, US) Surveys of Practice (Europe, US) � � Limited quality data on Limited quality data on � � when when � � to initiate to initiate � Mehta et al Am J Nephrol 1999; Wright et al Anaesthesia 2003; Ronco et al NDT 2001; Ricci et al NDT 2006; Hyman et al Am J Nephrol 2002; Adhikari, personal communication
� Biologic rationale Biologic rationale � � Consistency of findings across studies Consistency of findings across studies � � Early RRT (however defined) contributes to: Early RRT (however defined) contributes to: � � Improved survival � Improved survival � Improved renal recovery (to dialysis independence) � Improved renal recovery (to dialysis independence) � Shorter duration of RRT support � Shorter duration of RRT support � Reduced lengths of stay in ICU � Reduced lengths of stay in ICU
� Pre Pre- -morbid kidney function (i.e. Kidney reserve) morbid kidney function (i.e. Kidney reserve) � � Current kidney function Current kidney function � � Expected demand on kidney capacity Expected demand on kidney capacity � � Goals for clinical management Goals for clinical management � � Prevention Prevention of organ dysfunction of organ dysfunction � � Uremic toxicity � Uremic toxicity � Other organ toxicity (i.e. ARDS) � Other organ toxicity (i.e. ARDS) � Modulate organ � Modulate organ � � cross cross- -talk talk � � � i.e. Lung � i.e. Lung- -Kidney, Heart Kidney, Heart- -kidney kidney
� Logistics/organization Logistics/organization � � Country � Country � Type of institution � Type of institution � Type of ICU � Type of ICU � Service providing RRT � Service providing RRT � Individual practice/local culture � Individual practice/local culture � Resources/costs � Resources/costs
� Theoretical Advantages: Theoretical Advantages: � � Uremic/metabolic control � Uremic/metabolic control � Volume control � Volume control � Acid � Acid- -base homeostasis base homeostasis � Non � Non- -renal organ function renal organ function � Mitigate inflammation/oxidative stress � Mitigate inflammation/oxidative stress � Improved clinical outcomes (i.e. survival) � Improved clinical outcomes (i.e. survival)
Theoretical Better Uremic Control 45 Urea (mmol/L) 40 Late start 30 25 20 Early start 15 0 10 15 20 25 30 35 40 Days
� Theoretical drawbacks: Theoretical drawbacks: � � Need for catheter insertion � Need for catheter insertion � Potential for catheter � Potential for catheter- -related infection related infection � Exposure to extracorporeal circuit � Exposure to extracorporeal circuit � Potential unnecessary exposure to RRT � Potential unnecessary exposure to RRT
Study Year Patients Serum Urea (mmol/L) Mortality (%) Early Late Early Late Parsons 1964 33 48 71 25 88 Fischer 1966 162 54 82 51 77 Kleinknecht 1972 320 33 59 29 42 Conger 1975 18 18 43 20 64 Lange 1987 36 <29 >29 43 67 Gettings 1999 100 15 34 61 80 Tsai 2005 98 <80 >80 63 97
Critically Ill Trauma: Biochemistry 40 Late ~ Mortality 80% Urea (mmol/L) 30 20 Early ~ Mortality 61% 10 0 0 5 10 15 20 25 Days of CRRT Gettings et al ICM 1999
� 2 small single centre 2 small single centre � retrospective studies retrospective studies � Early: for oliguria � Early: for oliguria (<100ml/8hrs) (<100ml/8hrs) � Late: conventional � Late: conventional indications indications RRT started earlier after � RRT started earlier after � surgery in � � early early � � surgery in � Shorter stay in ICU Shorter stay in ICU � � Survival benefit Survival benefit � Demirkilic et al J Card Surg 2004; Elahi et al Eur J Cardiothora Demirkilic et al J Card Surg 2004; Elahi et al Eur J Cardiothorac Surg 2004 c Surg 2004
Urea � Urea <27 27 p n-=243 mmol/L mmol/L Urea (mmol/L) 17 41 <0.001 Adjusted RR 1.85 (95% CI 1.16-2.96) <0.001 Creatinine (umol/L) 301 415 No. Organ Failures 4 3 0.008 Sepsis (%) 37 46 0.14 Initial RRT (CRRT) (%) 69 43 0.001 Mortality (%) 0.09 Day 14 20 25 Day 28 35 41 Liu et al CJASN 2006
Hospital Mortality Stratified by Timing of implementation of RRT Hospital Mortality Stratified by Timing of implementation of RRT � � � � Late Late � � by Urea: by Urea: � Longer duration RRT � Longer duration RRT � Higher rate of non � Higher rate of non- -recovery recovery � Longer stay in hospital � Longer stay in hospital � � � Late Late � � by Creatinine by Creatinine � � Longer duration RRT � Longer duration RRT � Higher rate of non � Higher rate of non- -recovery recovery Bagshaw et al J Crit Care 2008
RCT: RR 0.64 (95% CI, 0.40-1.05) Cohort: RR 0.72 (95% CI, 0.64-0.82) Seabra et al AJKD 2008
What Modality of therapy? � The process of decision making is linked to indications leading to therapy initiation � Classic Blood Purification � Alternative � Fluid overload Ultrafiltration � Sepsis HVHF - CPFA
Study Year N Population Mortality (%) Fluid Overload (%FO) Survivors Non-Survivors Goldstein 2001 21 Pediatric CVVH 57 16.4% 34% Foland 2004 113 Pediatric CVVH 39 7.8% 15.1% Gillespie 2004 77 Pediatric CVVH 50 %FO >10 (median) HR 3.02, 95% CI 1.5-6.1, p=0.002 Goldstein 2005 116 Pediatric CVVH 48 14.2 25.4 Payen 2008 1,120 Adult AKI 36 (+) Fluid Balance (per 1L/24hr) HR 1.21, 95% CI 1.1-1.3, p<0.001
Gillespie et al Pediatric Nephrol 2004
NEFROINT PREVIEW
IRA SECTION � RIFLE CRITERIA � AKIN CRITERIA
IRA SECTION � RIFLE CRITERIA � AKIN CRITERIA
RIFLE ALERT RIFLE Alert Confirm Baseline Creatinine = 0.9 You reached RIFLE class � � RISK � � You reached RIFLE class RISK Actual creatinine = 1.55 x Baseline
Recommend





More recommend
Explore More Topics
Stay informed with curated content and fresh updates.