Drug-free Interventions to Reduce Pain or Opioid Consumption - PowerPoint PPT Presentation
1 Drug-free Interventions to Reduce Pain or Opioid Consumption Following Total Knee Arthroplasty. A Meta-Analysis. Dario Tedesco, MD, PhD candidate Postdoctoral Research Fellow Stanford University, Department of Medicine Center for
1 Drug-free Interventions to Reduce Pain or Opioid Consumption Following Total Knee Arthroplasty. A Meta-Analysis. Dario Tedesco, MD, PhD candidate Postdoctoral Research Fellow Stanford University, Department of Medicine Center for Biomedical Informatics Research
Disclosures 2 This project was supported by grant number R01HS024096 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. The contents of this work do not represent the views of the U.S. Department of Veterans Affairs or the United States Government. This research was also partially supported by the University of Bologna, Italy. No conflicts of interest to declare.
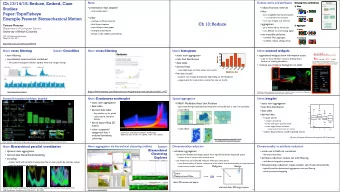
Outline 3 • Background: Total Knee Arthroplasty (TKA) and non- pharmacological therapies • Study and methods • Quality of evidence and main findings • Conclusions • Policy Impact
Background 4 • TKA is one of the most performed surgeries in the U.S. with about 675,000 procedures/year and $13B total annual cost. • First line of treatment is pharmaceutical (local anesthetics, systemic opioids and NSAIDs). However, many non-drug interventions are used for TKA pain management. • Conventional postoperative physical therapy is considered the gold standard for functional recovery and pain management. Steiner et al., 2012; Cram et al., 2012.
Background 5 • The current opioid epidemic termed the “worst drug crisis” in America. Opioid overdoses are leading cause of accidental death, with about 33,000 deaths in 2015. • Surgery is seen as gateway to opioid addiction. • Chronic use of opioids is associated with higher risk of postoperative morbidity and mortality after TKA. Rudd RA et al., 2016; Zywiel et al., 2011; Waljee et al., 2017; Abbasi 2016.
6 Study and methods
Aim of the study 7 Which of the most common drug-free interventions for TKA postoperative pain management are effective?
Study selection 8 Data sources: Medline, Embase, Cochrane Database of Systematic Reviews, Web of Science, Physiotherapy Evidence, and ClinicalTrials.gov, reference lists hand- searching. • 5,509 abstracts screened • 120 abstracts considered appropriate for assessment • Data extracted from 39 RCTs for meta-analysis • Included studies published between 1991 and 2015 • Only studies published in English
Interventions 9 Five most common non-pharmacological interventions for postoperative pain following TKA in scientific literature: • Acupuncture • Continuous Passive Motion • Cryotherapy • Electrotherapy • Preoperative exercise
Outcomes 10 Measurements of effectiveness: • Pain relief Visual Analogue Score (VAS) Score - WOMAC Score - • Opioid consumption Morphine equivalents (mg/Kg/48h) - Time to first Patient Controlled Analgesia (PCA) (minutes) -
11 Quality of evidence and main findings
Quality of evidence: the GRADE tool 12 GRADE is the Cochrane collaboration’s recommended approach for grading the quality of evidence through 5 criteria: • Risk of bias • Inconsistency • Indirectness • Imprecision • Publication bias Guyatt et al, 2011.
Quality of evidence 13 Outcome Publication Risk of bias Inconsistency Indirectness Imprecision GRADE bias Intervention Opioid consumption ⊕ CPM Serious Serious Not Serious Serious Not Serious Very Low ⊕ Cryotherapy Serious Serious Not Serious Not Serious Serious Very Low ⊕⊕⊕ Electrotherapy Serious Not Serious Not Serious Not Serious Not Serious Moderate ⊕⊕ Acupuncture Serious Serious Not Serious Not Serious Not Serious Low NSAID consumption ⊕ Cryotherapy Very Serious Serious Not Serious Serious Not Serious Very Low Time to first PCA ⊕⊕⊕ Acupuncture Serious Not Serious Not Serious Not Serious Not Serious Moderate
Quality of evidence 14 Outcome Publication Risk of bias Inconsistency Indirectness Imprecision GRADE Intervention bias Pain relief – VAS ⊕ CPM Very Serious Not Serious Not Serious Serious Not Serious Very Low ⊕ Cryotherapy Very Serious Serious Not Serious Not Serious Serious Very Low ⊕ Electrotherapy Very Serious Serious Not Serious Not Serious Serious Very Low ⊕⊕ Acupuncture Serious Serious Not Serious Not Serious Not Serious Low Pain relief – WOMAC ⊕⊕ CPM Very Serious Not Serious Not Serious Not Serious Not Serious Low ⊕⊕ Preoperative Serious Serious Not Serious Not Serious Not Serious exercise Low
Electrotherapy: opioid consumption 15 Morphine equivalents mg/Kg/48h Level of evidence: ⊕⊕⊕ Moderate
Acupuncture: opioid consumption 16 Time to first PCA (minutes) � Level of evidence: ⊕⊕⊕ Moderate
Electrotherapy: pain relief 17 Level of evidence: ⊕ Very Low VAS score mean differences
Acupuncture: pain relief 18 VAS score mean differences Level of evidence: ⊕⊕ Low
Findings 19 Moderate-certainty evidence • Electrotherapy and acupuncture reduce/delay opioid consumption. Low/very low certainty-evidence • Electrotherapy and acupuncture improve pain. • Continuous passive motion and preoperative exercise do not improve pain or reduce opioid consumption. Very low-certainty evidence • Cryotherapy reduces opioid consumption, but does not improve pain.
Conclusions 20 • Following TKA, there is moderate evidence that Electrotherapy and Acupuncture are associated with modest but clinically significant reduction and delay in opioid consumption. • However, there was low/very low evidence that Electrotherapy and Acupuncture improve pain. • The quality of evidence for other interventions on pain management was low/very low. • Given the current opioid crisis, more high-quality studies on non-drug interventions are needed.
Policy impact 21 • Electrotherapy and Acupuncture can be part of evidence-based guidelines for pain management in patients undergone TKA. • More funding and initiatives are needed to support non- pharmaceutical pain management strategies. • Quality metrics should be developed around the use of non- pharmaceutical pain management strategies. • Common interventions such as Continuous Passive Motion and Cryotherapy for pain management still lack evidence and should be adopted with caution.
Acknowledgments 22 Thanks to my amazing mentors and colleagues: Mentor and PI: Tina Hernandez-Boussard, PhD, MPH Mentor: Maria Pia Fantini, MD Colleagues: • Davide Gori, MD • Karishma Desai, PhD • Steven Asch, MD, MPH • Catherine Curtin, MD • Ian Carroll, MD • Kathryn McDonald, PhD
23 Questions? Contact: dariot@stanford.edu
Recommend










More recommend
Explore More Topics
Stay informed with curated content and fresh updates.