Oxford Splash 2019 Diabetes: how to fight an epidemic Matthew Lloyd Lesson goals • Gain a basic understanding of the pathology and treatment of the major types of diabetes • Consider the trends in diabetes and obesity prevalence and the associated costs and discuss what can be done to address them
What is diabetes? Diabetes is defined by its symptoms (high blood glucose). It is actually a group of diseases with di ff erent causes and requiring di ff erent treatments Characterised by recurrent or persistent hyperglycaemia . Diagnostic criteria include fasting blood glucose ≥ 7 mmol/L or glycated haemoglobin ≥ 6.5% May be caused by insu ffi cient insulin secretion , insulin sensitivity or both Nearly all cases are type I or type II . There are also rare hereditary forms , and some women experience temporary gestational diabetes during pregnancy Complications of diabetes can be serious, reducing life expectancy by >10 years in type I and up to 10 years in type II Normal fasting blood glucose is 4-6 mmol/L
How is blood glucose regulated? Plasma glucose (PG) homeostasis is a balancing act. Levels should be maintained in a safe range of approximately 4-6 mmol/L Stimulus: rising PG Stimulus: falling PG Response: glucagon secretion Response: peripheral Response: glucose uptake insulin secretion Response: liver Response: liver glycogen breakdown glucose uptake and and glucose release glycogen synthesis Organ that takes up most glucose in response to insulin is skeletal muscle – it’s a major energy user and glycogen store
How is blood glucose regulated?
How is blood glucose regulated? Endocrine tissue of pancreas Islets constitute only 1-2% of pancreas volume but receive 10–15% of its blood flow Pancreas is unusual as it is both an endocrine and exocrine organ! Islets of Langerhans contain two cell types that directly sense glucose levels and respond by altering their secretion of hormones. Beta cells secrete insulin and alpha cells glucagon. Note: somatostatin produced by delta cells has regulatory action within islet (inhibits insulin secretion) but you don’t need to know this.
Types of diabetes Proportion of Type Cause Onset Treatment diabetics Autoimmune Sudden, usually in destruction of Type I childhood or 5-10% Insulin replacement pancreatic beta adolescence cells Insulin resistance Gradual, late Lifestyle changes, and insu ffi cient Type 2 childhood to old 90-95% drug and/or insulin compensatory age therapy secretion Mutations a ff ecting Sudden, aged <6 Neonatal insulin secretion <1% Sulfonylurea drugs months (but not synthesis) Maturity onset A variety of Drug or insulin Gradual, usually diabetes of the mutations in 1-2% therapy (depending aged <30 metabolic genes on cayse) young (MODY) Type II (T2DM) is most common form, and the only form that is currently preventable Note: insulin resistance may be present for 10-20 years before clinical onset of type II diabetes. This period is called pre-diabetes. Main focus will be on type 2 as this is gives us the greatest potential for reducing the global disease burden.
T2DM Pathology and Risk Factors Obesity is the main risk factor 20% Other risk factors include: • Age >45 • South Asian, East Asian, Pacific Islander, Native American, Latino, or African ethnicity • Family history of T2DM 80% Obesity Other ~30% of UK population is obese ~10% of UK adults have T2DM This is a public health crisis! But why such a strong association with obesity? Increasing obesity prevalence is primary driver of increasing T2DM incidence, as reflected by the strong positive correlation between BMI and diabetes risk. Note: caucasians have lowest risk of developing diabetes for a given BMI. Perhaps because have had longest to adapt to high carbohydrate diet?
T2DM Cause and Progression Compensatory Relative deficiency Absolute deficiency of Insulin resistance increase in insulin of insulin secretion insulin secretion (loss secretion (decompensation) of beta cell function) Result: dramatic swings between hyperglycaemia and hypoglycaemia But how does insulin resistance arise in the first place? Beta-cell function is already reduced by half by time of diagnosis – becomes increasingly di ffi cult to reverse diabetes so important to intervene early. Note: hyperglycaemia is exacerbated by increased basal glucagon secretion, leading to inappropriate glucose release by liver after a meal. Conversely, glucagon may be too low overnight, leading to fasting hypoglycaemia
T2DM Cause and Progression Regulation of fat metabolism and carbohydrate metabolism is highly integrated. Defects in fat metabolism probably precede insulin resistance Glycogen storage capacity is limited. Following a carbohydrate-rich meal, e xcess glucose is converted to fat Inactivity increases fat deposition, whereas exercise increases capacity of muscle to take up and use glucose and improves mitochondrial function When safe storage capacity for fat is exceeded, fat is stored in unsuitable tissues e.g. liver and muscle Fat is metabolised in preference to glucose, leading to reduced glucose uptake Chronic inflammation may contribute to disease development Metabolic syndrome is characterised by abdominal obesity, high blood pressure, high blood sugar, high serum triglycerides (fats), and low serum HDL (“good cholesterol”)
T2DM Cause and Progression This diagram summarises the factors that contribute to T2DM development. I’ve highlighted in red the causes that cannot be controlled, and in green those where people have the power to make positive choices.
Complications of diabetes If blood glucose levels are not properly controlled by treatment, diabetes can have life-threatening complications Cause of death in 50% type II diabetics In 2012, 79% of NHS diabetes spending was on treating complications Microvascular and macrovascular disease: high blood glucose damages blood vessels (e.g. through atherosclerosis) and other tissues Note: gestational diabetes increases risk of heart disease in newborn
Recap Quiz How many types of diabetes are there? A. 1 B. 2 C. 4 D. >4 Which hormones oppose the e ff ects of insulin? Choose as many as you think are correct A. Cortisol B. Glucagon C. Adiponectin D. Adrenaline Which organs are capable of sensing blood glucose levels? Choose as many as you think are correct A. Brain B. Intestine C. Pancreas D. Liver Write down your answers and put your name at the top. I will announce the top scorer(s) at the end of the class. How many types of diabetes are there? >4 Which hormones oppose the e ff ects of insulin? Glucagon, adrenaline, cortisol – these promote the use of energy stores, whereas insulin and adiponectin promote the uptake and storage of glucose from food Which organs are capable of sensing blood glucose levels? Pancreas (beta and alpha cells), intestine (gut L cells secrete GLP-1 and other peptide hormones) and brain (hypothalamus contains specialised neurons that sense glucose and play a role in regulating pancreatic insulin secretion and appetite). Note that liver metabolism is regulated by PG, but it is not a precise sensor (does not involve electrically active cells)
Recap Quiz Can you identify the complications of diabetes and avoid the decoys? Choose as many as you think are correct A. Nephropathy B. Osteopathy C. Psychopathy D. Neuropathy Which tissues are major glycogen stores? Choose as many as you think are correct A. Pancreas B. Liver C. Cardiac muscle D. Skeletal muscle Can you identify the complications of diabetes? Retinopathy (can lead to blindness), neuropathy (nerve damage), nephropathy (kidney damage/failure), stroke, CVD are all complications of diabetes Which tissues are major glycogen stores? Skeletal muscle, liver and cardiac muscle. Pancreas does not store significant amounts of glycogen in healthy people, but it is found in beta cells from diabetic donors and animals
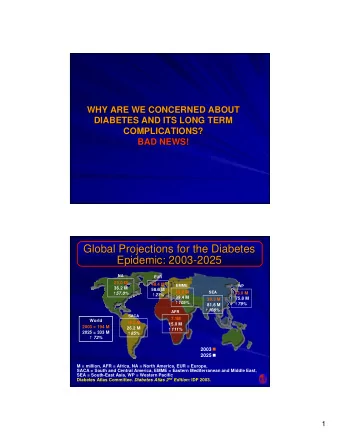
A Global Crisis Europe actually has lower diabetes prevalence than most of world, probably due to lower genetic susceptibility as well as lifestyle factors. Note: significant numbers live with undiagnosed diabetes, which increases danger of complications
Treatments for T2DM Lifestyle modification: l ess sugar in diet, more exercise , balancing caloric intake and expenditure First-line pharmaceutical treatment: metformin Regulation of blood cholesterol Drugs that enhance insulin secretion : sulfonylureas, incretin mimetics and DPP-4 inhibitors (gliptins) Insulin therapy (when endogenous production fails) Bariatric surgery Current NICE guidelines are to gradually intensify drug regimen (both in terms of dosage and number of drugs), while advising lifestyle changes Too few people succeed in making their lifestyle healthier. Do we need a more radical approach to incentivise change ? Not fully understood how metformin works, but decreases glucose production by the liver and increases insulin sensitivity of body tissues Note undesirable side e ff ects to some drugs e.g. weight gain, increased pancreatic cancer risk Bariatric surgery very e ff ective due to substantial weight loss
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries