Insulin Speakers Dr Roni Saha , Consultant Diabetologist, St George’s Hospital Lisa Egan, Community Diabetic Specialist Nurse, CLCH In collaboration with the Health Innovation Network
Agenda TIME ACTIVITY FORMAT 12.30 – 13.00 LUNCH 13.00 – 13.05 Introductions Presentation The Diabetes problem… Presentation + interactive The right time for insulin; an Presentation evidence & case-based discussion Myths and barriers Insulin Management: Key Facts Presentation Insulin initiation The right insulin Insulin types & regimens Insulin dose adjustment Cases, conclusions & questions Presentation + interactive 14.55 – 15.00 Evaluation Sheet Completion Attendees
Introductions Putting faces to names: Dr Roni Saha (Consultant Diabetologist, SGH) Dr Sachin Patel (West Wandsworth Diabetes GP Lead) Raj Dhir (Senior Prescribing Advisor, Wandsworth CCG) Diabetes Specialist Nurses (CAHS and QMH) Vedrana van Rheede (Project Manager, GP Federation) Pamela Wilson (Coordinator, GP Federation)
Diabetes Service Improvement in Primary Care • Wandsworth CCG has commissioned BHCIC/GP Federation to undertake a review of diabetes care, based on the success of the 2017/2018 Diabetes deep dives • Overarching aim is to review and improve service pathways as an opportunity to improve clinical outcomes for patients with Diabetes
Elements of the review • Primary Care activity including Deep Dive visits • Clinical Audit of Diabetic patients (as under PACT service req. 10) • Education needs • Outpatient activity review • Education events
Diabetes related activities and events • PACT Diabetes Clinical Audit (part of PACT Service Specification req.10) Part 1 audit due 31 st July 2018. • 20 th September 2018 Event focusing on the initial audit and outcomes • Part 2 audit due end January 2019 • Third Diabetes related event to be confirmed between February- March 2019.
The Diabetes Problem…
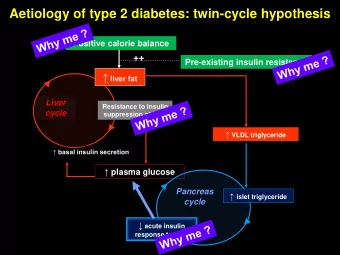
Pathophysiology of type 2 diabetes involves three core defects and multiple organ systems 3. Pancreatic 1. Peripheral tissues beta cells 2. Liver Decreased Decreased Increased lipolysis Increased insulin secretion glucose uptake glucose production Pancreatic alpha cells Excessive glucagon secretion Insulin Islet cell resistance dysfunction Combined islet cell dysfunction and insulin resistance HYPERGLYCAEMIA 1. Inzucchi SE. JAMA 2002;287:360 – 372 . DIAB-1150856-0000 2. Porte D Jr, Kahn SE. Clin Invest Med 1995;18:247-254.
The ominous octet: Multiple organ and hormone dysfunctions contribute to type 2 diabetes β Glucose Insulin production secretion α Glucagon Glucose secretion uptake Chronic hyperglycaemia Incretin Lipolysis effect Glucose Neurotransmitter reabsorption dysfunction DIAB-1150856-0000 1. DeFronzo RA (2009) Diabetes 58 : 773 – 95
Islet cell dysfunction in type 2 diabetes Normal Type 2 diabetes • Fewer islets Alpha cells • Fewer beta cells per islet Glucagon Pancreas Pancreas Beta cells Insulin Cell type Hormone Physiological action Abnormality in type 2 diabetes Alpha cell Glucagon Stimulates hepatic glucose output to avoid Glucagon not suppressed after eating; worsens hypoglycaemia hyperglycaemia Beta cell Increases glucose uptake in the liver and Inadequate and delayed insulin response contributes Insulin peripheral tissues to hyperglycaemia 1. Porte D Jr, Kahn SE. Clin Invest Med 1995;18:247-254. 2. Rhodes CJ. Science 2005; 307:380-384. 3. Gerich JE. International Rev Phys 1981; 24:243-275. 4. Müller WA et al. N Engl J Med 1970: 283:109-115. 11 DIAB-1150856-0000 Illustration reproduced with permission from reference 2.
Diabetes is a chronic and progressive disease ▪ Decline in insulin sensitivity, β -cell function and incretin effects all occur prior to development of overt type 2 diabetes 250 Relative Amount Insulin resistance 200 150 ≥50% loss of β -cell function at diagnosis* 100 Insulin level 50 β -cell function 0 Diabetes Onset 350 Postmeal glucose Diagnosed Glucose (mg/dL) 300 Prediabetes diabetes 250 Fasting glucose 200 150 100 50 -15 -10 -5 0 5 10 15 20 25 30 Years Adapted from Kendall DM et al (2009) Am J Med 122 :S37 – 50. *By the time diabetes is clinically diagnosed, β - cell function may be reduced by ≥50%; subjects in the upper tertile of IGT are near- maximally insulin resistant and have lost more than 80% of their β -cell function. 1 – 3 Representative depiction of the natural progression of type 2 diabetes (time course and function). 1 IGT=impaired glucose tolerance. 1. Kendall DM et al (2009) Am J Med 122 : S37 – 50; 2. DeFronzo RA (2009) Diabetes 58 : 773 – 95; DIAB-1150856-0000 3. Holman RR (1998) Diab Res Clin Prac 40 (suppl):S21 – 5
Impact of intensive therapy for diabetes: Summary of major clinical trials Study Microvascular Macrovascular Mortality UKPDS 1,2 ACCORD 3 – 5 NR * ADVANCE 6,7 NR VADT 8,9 Initial trial Long-term follow-up *End-stage renal disease. ACCORD=Action to Control Cardiovascular Risk in Diabetes; ADVANCE=Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation; NR=not reported; UKPDS=UK Prospective Diabetes Study; VADT=Veterans Affairs Diabetes Trial. 1. UKPDS (1998) Lancet 352 : 837 – 53; 2. Holman RR et al (2008) N Engl J Med 359 : 1577 – 89; 3. Gerstein HC et al (2008) N Engl J Med 358 : 2545 – 59; 4. ACCORD Study Group (2011) N Engl J Med 364 : 818 – 28; 5. Ismail-Beigi F et al (2010) Lancet 376 : 419 – 30; 6. Patel A et al (2008) N Engl J Med 358 : 2560 – 72; 7. Zoungas S et al (2014) N Engl J Med 371 : 1392 – 406; 8. Duckworth W et al (2009) N Engl J Med 360 : 129 – 39; 9. Hayward RA et al (2015) N Engl J Med 372 : 2197 – 206
HbA1c individual target setting Functionally dependent, frail, limited life Considering a second At diagnosis Discuss with the expectancy or third agent individual History of severe hypoglycemia On no / one oral agent Advanced microvascular or macrovascular complications Extensive comorbid conditions Over time 58mmol/mol 48mmol/mol 53mmol/mol 58- 64mmol/mol 7.5% 7.5-8% 7% 6.5% or higher UKPDS (1998): mean [UKPDS: mean HbA1c in control group - 63mmol/mol HbA1c in the intensive group 53mmol/mol Preferred target if taking NICE QS6 (offer dual therapy) sulfonylureas NICE NG28 (2015) ADA/EASD position statement update (Inzucchi et al. 2015) Currie et al. (2010) Survival as a SIGN (2010) Diabetes UK steering group (2013). Clinical care function of HBA1c in people with recommendations: end of life diabetes care ADA/EASD position type 2 diabetes: a retrospective analysis, Lancet, 375: 481-489 NICE NG28 (2015) statement update (Inzucchi Abdelhafiz & Sinclair (2016) Frailty & hypoglycaemia in older people with type 2 diabetes, J of Diabetes et al. 2015) NHS England measure Nursing 20(9): 330-331 NICE NG28 (2015)
Glycaemic goals for people with T2DM Suggested Goals for Glycemic Treatment in Patients with Type 2 Diabetes.
The Right Time for Insulin: An Evidence & Case Based Discussion
Some patients with T2DM may not benefit from insulin • Some obese people in whom insulin treatment can lead to further weight gain, with little or no improvement in HbA1c • People whose oral anti-diabetes treatment regimen could be improved • Elderly people with a short duration of diabetes and no symptoms of hyperglycaemia • People with other physical or mental health problems in whom the potential benefits of insulin treatment may not outweigh the potential risks • Occupational related • Royal College of Nursing (2007) Starting insulin treatment in adults with type 2 diabetes. RCN guidance for nurses. Available at: http://tiny.cc/4aktx(accessed 04.02.2013)
Insulin use in Type 2 Diabetes • UKPDS - Type 2 diabetes is a progressive condition 1 • At diagnosis, beta cell function may be reduced by 50%. This decline continues regardless of therapy 2 • Some patients will progress to insulin therapy more quickly than others, depending on duration of diagnosis 1. UKPDS (49).Jama 1999;281(21):2005-12 Williams G & Pickup JC. Handbook of Diabetes, 3 rd Ed. 2004 2.
Question: What target would you recommend for this person? 50-year-old lady, 10-year history of type 2 diabetes, with an HbA 1c level of 8.6% (70 mmol/mol) on max metformin, sulphonylurea and GLP-1 agonist 1.<6.5% (<48 mmol/mol) 2.<7.0% (<53 mmol/mol) 3.<7.5% (<58 mmol/mol) 4.<8.0% (<64 mmol/mol) 5.<8.5% (<69 mmol/mol) 6. I’m happy with her current HbA 1c level 7.Something else
Question: What target would you recommend for this person? 50-year-old lady, 10-year history of type 2 diabetes, with an HbA 1c level of 8.6% (70 mmol/mol) on max metformin, sulphonylurea and GLP-1 agonist 1.<6.5% (<48 mmol/mol) 2.<7.0% (<53 mmol/mol) 3.<7.5% (<58 mmol/mol) 4.<8.0% (<64 mmol/mol) 5.<8.5% (<69 mmol/mol) 6. I’m happy with her current HbA 1c level 7.Something else 53mmol/mol
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries