2/ 6/ 2020 Bacterial Endocarditis Henry F. Chambers, MD No disclosures 1
2/ 6/ 2020 Topics for Discussion • Pathophysiology • Epidemiology • Diagnosis • Treatment and Management Pathophysiology 2
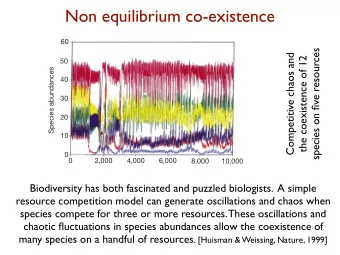
2/ 6/ 2020 Primary Lesion: Valvular Vegetation Valvular Infected Platelet-fibrin Non-bacterial Adherence, Endothelium vegetation colonization deposition at thrombotic site of injury endocarditis Bacteremia Trauma, Valve destruction turbulent Continuous bacteremia, blood flow, metastatic infections etc Embolization Immune complexes Mitral Valve Vegetation 3
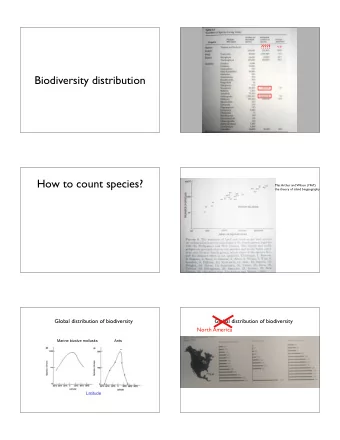
2/ 6/ 2020 Vegetation Histopathology Metastatic Infection Osteomyelitis 4
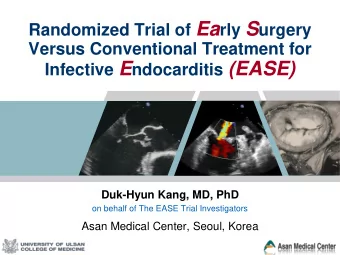
2/ 6/ 2020 Systemic Embolization Renal Infarct CNS Septic Pulmonary Emboli 5
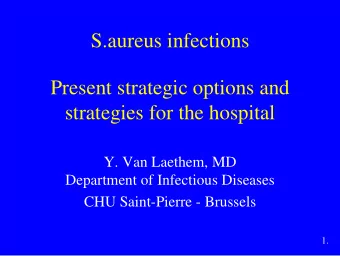
2/ 6/ 2020 Microvascular Emboli Osler ’s node Petec hiae Splinter hemor r hages R oth spots Immune-complex Glomerulonephritis 6
2/ 6/ 2020 Epidemiology Which one of the following statements is correct? 1. Staphylococcus aureus is the most common cause of bacterial endocarditis 2. Dental procedures carry a substantial risk for streptococcal endocarditis for patients with predisposing cardiac lesions 3. Three-quarters of patients with endocarditis have a known underlying cardiac predisposing condition 4. Fever and a new cardiac murmur are present in the majority of patients with endocarditis 7
2/ 6/ 2020 Epidemiology 3-15/ 100,000 pe rso n-ye ars Cahill, Lancet 2016; 387: 882 Microbiology Organisms Approximate % of Total Staphylococci 40-50 S. aureus 30-40 Coag-neg 10 Streptococci 25-30 Viridans group 20 S. gallolyticus 5 Groups B, C, D 5 Enterococcus 10 HACEK 1-2 Culture-negative 3-5 Arch Intern Med. 2009;169:463; Antimicrob Agents Chemother. 2015;60:1411; Clin Infect Dis. 2018;66:104; Lancet 2016; 387: 882 8
2/ 6/ 2020 Culture-Negative Endocarditis • Prior antibiotics • Fastidious organisms – HACEK – Abiotrophia defectiva, et al • “ Non-cultivatable ” organism – Bartonella quintana – Coxiella burnetii , Chlamydophila psittaci , Trophyrema whippelii , Legionella sp • Fungi (molds) • Not endocarditis – Libman-Sacks, myxoma, APLS, marantic Risk Factors • Community-acquired or hospital associated • Previous endocarditis • Injection drug use • Hemodialysis • Prosthetic valve, implanted intracardiac device • Underlying congenital or valvular heart disease • Poor dental hygiene or dental procedures? 9
2/ 6/ 2020 Clinical Signs and Symptoms Finding Approximate Prevalence, % Fever 90 Murmur 70-85 New murmur 50 Worsening old murmur 20 Peripheral stigmata (e.g., Osler’s) 20% or less Heart failure, cardiac complications 20-50 CNS complications 20-40 Risk of Endocarditis Following an At-Risk Dental Procedure Predisposing Prophylaxis Risk of condition Endocarditis Prosthetic valve No 1/10,700 Native valve No 1/46,000 PV or NV Yes 1/149,000 Duval, Clinical Infectious Diseases 2006; 42:e102–7 10
2/ 6/ 2020 AHA Guidelines: Prevention of Endocarditis • Prosthetic valve • Previous infective endocarditis • Congenital heart disease – Unrepaired – Within 6 mo of repair – Incomplete repair • Transplant cardiac valvulopathy Circulation. 2007;116:1736-1754 Diagnosis 11
2/ 6/ 2020 Which one of the following is a major criterion for the diagnosis of endocarditis? 1. Worsening or changing regurgitant murmur 2. Two separate blood cultures positive for S. aureus, viridans strep, or HACEK organism 3. “Shaggy” appearance of the valve on transesophageal echocardiogram 4. Presence of Osler’s node Modified Duke Criteria • Pathologic criteria – Histopathologic evidence of endocarditis – Microorganisms on the valve or culture of it • Major clinical criteria – Positive blood cultures*: a) typical organisms or b) persistently positive cultures if not typical ones – Evidence of endocardial involvement: a) positive echocardiogram or b) new regurgitant murmur • Minor clinical criteria: – Temp > 38, IVDU, predisposing cardiac lesion, vascular phenomena, immunologic phenomena, blood culture or serological evidence of infection not meeting major criteria * Coxiella burnetti antiphase 1 IgG titer > 1:800 also counts 12
2/ 6/ 2020 Endocarditis • Definite endocarditis – Pathologic criteria or – Clinical criteria • Two major clinical criteria ( i.e., ECHO + culture) or • One major and three minor criteria or • Five minor criteria • Possible endocarditis – One major + one minor criteria or – Three minor criteria Sensitivity of ~80%, higher if “possible” are included, lower for PVE, culture-negative, cardiac device infection, R-sided endocarditis Not Endocarditis • Alternative diagnosis made • Clinical resolution with < 4 days of antibiotic therapy • No pathological evidence found at surgery or autopsy after < 4 days of antibiotic therapy • Clinical criteria for possible or definite endocarditis not met 13
2/ 6/ 2020 Role of Echocardiograpy SUSPECTED ENDOCARDITIS High risk patient or moderate Low risk patient to high clinical suspicion, & low clinical suspicion Initial TTE difficult imaging candidate TEE after TTE asap Neg Pos Rx Neg Pos Low High risk suspicion suspicion features on TTE Look for Rx Yes suspicion other No source TEE No Look for other TEE TEE source What is High Risk? • High risk patients (examples) – Prosthetic valve – Congenital heart disease – Previous endocarditis – New murmur, heart failure, heart block, stigmata of IE • High risk TTE (examples) – Large or mobile vegetations, anterior MV leaflet veg – Valvular insufficiency, perivalular extension, valve perforation – Ventricular dysfunction 14
2/ 6/ 2020 Harmonic TTE vs TEE for Diagnosis of IE - Conclusively negative harmonic TTE useful to r/o native valve IE - TTE less sensitive than TEE for detecting prosthetic IE vegetations, dehiscence, abscess - Indeterminant TTE not useful to r/o endocarditis - TTE insensitive for abscess, IE of implantable cardiac device - Specificity of TTE is ~95% Bai, J Am Soc Echocardiogr 2017; 30:639-646.e8 Other Diagnostic Modalities • 18 F-fluorodeoxyglucose-PET/CT – May be useful in PVE when TEE is non-diagnostic – May be useful for detecting metastatic infection – There are issues with specificity • Cardiac CT angiography – Less imaging artifact than TEE in PVE – Improved resolution of paravalvular complications – May be useful in PVE when TEE is non-diagnostic • Cardiac MRI? 15
2/ 6/ 2020 Tools for Diagnosis of Culture-Negative Endocarditis Organism Clinical clues Serology Specific Universal PCR 16s/18s rRNA PCR HACEK, strep, etc Prior antibiotics X Legionella Immunocompromise X X T. whipplei Chronic illness X X Brucella Travel X X Bartonella sp. Cats, homeless, lice X (>1:800) X X Mycoplasma X X Q fever Animal contact, lab X (>1:800) X X Chlamydia Bird exposure X X Treatment 16
2/ 6/ 2020 Circulation. 132:1435-86, 2015 Which of the following statements is correct concerning the use of gentamicin for treatment of bacterial endocarditis? 1. It should be used in combination with nafcillin for treatment of MSSA endocarditis 2. It should be used in combination with ampicillin or ceftriaxone for treatment of HACEK endocarditis 3. It should be used in combination with penicillin for treatment of penicillin-nonsuscepitble viridans strep endocarditis 4. It should be used to achieve satisfactory cure rates of enterococcal endocarditis 17
2/ 6/ 2020 Native Valve S. aureus IE Regimen Duration Comments MSSA Nafcillin or 6 wk 2 wk uncomplicated R- oxacillin sided IE (IDU) Cefazolin 6 wk Pen-allergic naf-intolerant patient (equivalent to naf) MRSA Vancomycin 6 wk For MSSA if beta-lactam hypersensitivity Daptomycin 6 wk > 8 mg/kg/day, vanco alternative No gentamicin, no rifampin Treatment of VGS and Strep. gallolyticus IE • Pen MIC < 0.12 μ g/ml – Penicillin, ceftriaxone, vancomycin x 4 weeks • Pen MIC > 0.12 μ g/ml, < 0.5 μ g/ml – Penicillin or ceftriaxone (4 wk) + gent (2 wk) – Ceftriaxone or vancomyin (4wk) • Pen MIC > 0.5 μ g/ml (and nutritionally deficient species) – Penicillin or ceftriaxone + gent – Vancomycin – Duration not defined (4 wk?) – ID consult 18
2/ 6/ 2020 Enterococcal Endocarditis Regimen Duration Comments (Strength of Rec) Pen or amp + gent 4-6 wk Pen S, Gent 1 mg/kg q8h, 6 wk for PVE, symptoms>3 mo Amp + Ceftriaxone 6 wk Pen S, Aminoglycoside susceptible or resistant Pen or amp + strep 4-6 wk Gent resistant, Strep synergy, ClCr > 50 Vanco + gent 6 wk Pen resistant or beta-lactam intolerant (toxic!) Linezolid or dapto > 6 wk VRE: Dapto 10-12 mg/kg & combo with amp or ceftaroline HACEK Organisms • Haemophilus species • Aggregatibacter species • Cardiobacterium hominis • Eikenella corrodens • Kingella species 19
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries