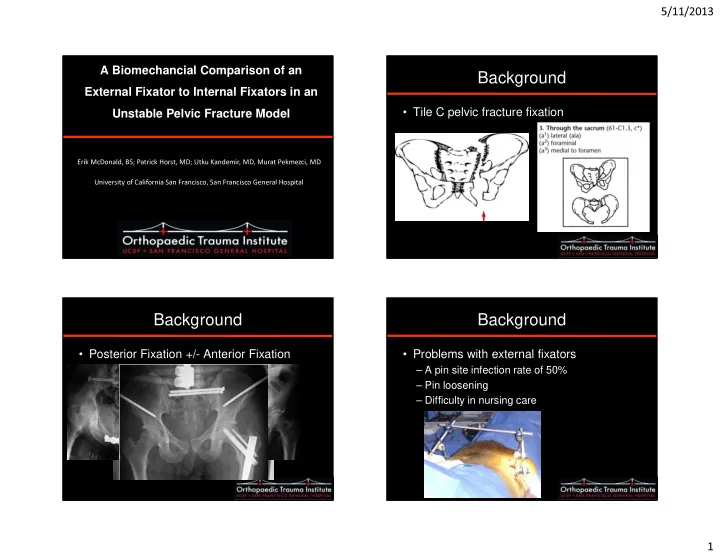
5/11/2013 A Biomechancial Comparison of an Background External Fixator to Internal Fixators in an Unstable Pelvic Fracture Model • Tile C pelvic fracture fixation Erik McDonald, BS; Patrick Horst, MD; Utku Kandemir, MD, Murat Pekmezci, MD University of California San Francisco, San Francisco General Hospital Background Background • Posterior Fixation +/- Anterior Fixation • Problems with external fixators – A pin site infection rate of 50% – Pin loosening – Difficulty in nursing care 1
5/11/2013 Anterior Internal Fixators Anterior Internal Fixators • Kuttner et al, 2009 Anterior Internal Fixators Purpose • To compare In-Fix to external fixator • To compare different configurations of In- Fix in an unstable sacral fracture with comminuted anterior ring injury model. 2
5/11/2013 Methods Methods • The following 4 anterior fixation techniques were • Synthetic sawbone pelvis (Sawbones, Vashon, WA) investigated: • Group I (ExFix): Supra-acetabular external fixation with were divided into two groups which received one of the following posterior fixation methods: 6.0mm pins • Group II (InFix): Supra-acetabular INFIX with 7.5mm • A single 7.0mm transsacral screw through the S1 pedicle screws body (TS) • Group III (Double InFix): Supra-acetabular Infix with two 7.5mm pedicle screws bilaterally, each connected by a rod • A single illiosacral screw through the S1 body (IS) • Group IV (Double InFix w/ CC): the addition of three cross connectors to the Double InFix configuration. Methods Methods Group II (In-Fix): Group I (Ex-Fix): Supra-acetabular Supra-acetabular INFIX with 7.5mm external fixation pedicle screws with 6.0mm pins 3
5/11/2013 Methods Methods Group III (Double Group IV (Double In-Fix): Supra- In-Fix w/ CC): the acetabular Infix addition of three with two 7.5mm cross connectors pedicle screws to the Double bilaterally, each InFix connected by a configuration. rod Test Protocol Test Protocol • All anterior fixation groups were • Three dimensional displacement and rotation was tested on each specimen with nondestructive loading by means measured using an optical tracking system. of a single leg stance model. • Peak to peak (P2P) displacement and rotation, • Condition displacement (CD), or settling • The specimens were subjected to 25 cycles of cyclic loading between 100 and 200N and then • Differences between outcome metrics between the loaded in displacement control to a maximum load of 300N. anterior fixation was analyzed using the a non- parametric repeat measures test with Dunn’s post hoc comparison with p<0.05 considered significant. 4
5/11/2013 Results Results Pubic Displacement Sacral Displacement 350 Pubic Displacement Sacral Displacement 3 Peak to Peak Elongation 4 2.5 Conditioning Elongation 300 2 3 (mm) 1.5 (mm) 2 250 1 1 0.5 Maximum Load (N) 0 0 200 InFix Double Cross InFix Double Cross Pubic Rotation Sacral Rotation 150 Pubic Rotation Sacral Rotation 0.6 Peak to Peak Elongation 2.5 Conditioning Elongation 0.5 100 2 0.4 (deg) 1.5 0.3 (deg) 1 0.2 50 0.5 0.1 0 0 0 InFix Double Cross InFix Double Cross ExFix InFix Double Cross The Ex-Fix group failed in 8/9 TS specimens, and 7/9 IS specimens Discussion • Construct Stiffness 5
5/11/2013 • 24 patients, Oct ’09-Jul ’10 • 2 LFCN palsy • 1 HO • No Loss of reduction Limitations Conclusions • Saw Bone Model • In-Fix is stronger than external fixation in an unstable – Cadaver model for higher loads pelvic fracture model when only one level of posterior fixation is implemented. • Using the same model for all constructs • Addition of another In-Fix or cross connectors did not result in less displacement or rotation over the Single In-Fix group. 6
5/11/2013 Conclusions • The improved biomechanical characteristics – Significant advantage for anterior pelvic ring fixation when traditional internal fixation is not an option. THANK YOU 7
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries