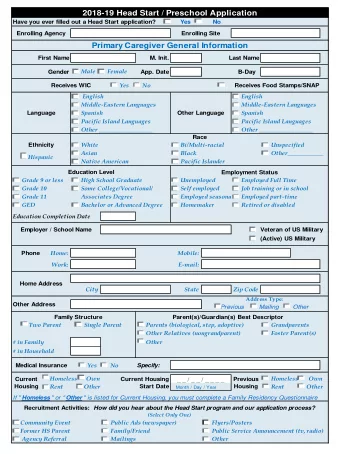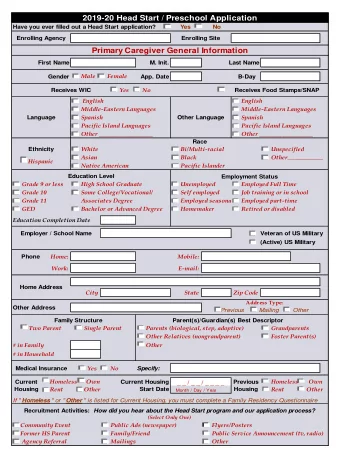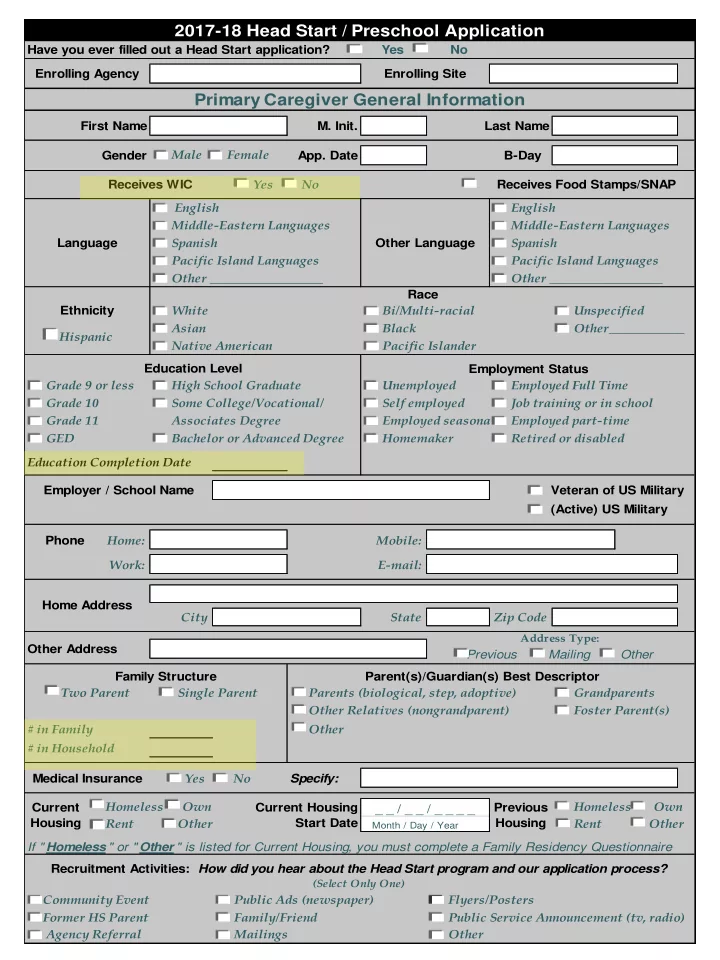
2017-18 Head Start / Preschool Application Have you ever filled out a Head Start application? Yes No Enrolling Agency Enrolling Site Primary Caregiver General Information First Name M. Init. Last Name Gender Male Female App. Date B-Day Receives WIC Yes No Receives Food Stamps/SNAP English English Middle-Eastern Languages Middle-Eastern Languages Language Spanish Other Language Spanish Pacific Island Languages Pacific Island Languages Other __________________ Other __________________ Race Ethnicity White Bi/Multi-racial Unspecified Asian Black Other____________ Hispanic Native American Pacific Islander Education Level Employment Status Grade 9 or less High School Graduate Unemployed Employed Full Time Grade 10 Some College/Vocational/ Self employed Job training or in school Grade 11 Associates Degree Employed seasonal Employed part-time GED Bachelor or Advanced Degree Homemaker Retired or disabled Education Completion Date Employer / School Name Veteran of US Military (Active) US Military Phone Home: Mobile: Work: E-mail: Home Address City State Zip Code Address Type: Other Address Previous Mailing Other Family Structure Parent(s)/Guardian(s) Best Descriptor Two Parent Single Parent Parents (biological, step, adoptive) Grandparents Other Relatives (nongrandparent) Foster Parent(s) # in Family Other # in Household Medical Insurance Yes No Specify: Current Homeless Own Current Housing Previous Homeless Own _ _ / _ _ / _ _ _ _ Housing Start Date Housing Rent Other Rent Other Month / Day / Year If " Homeless " or " Other " is listed for Current Housing, you must complete a Family Residency Questionnaire Recruitment Activities: How did you hear about the Head Start program and our application process? (Select Only One) Community Event Public Ads (newspaper) Flyers/Posters Former HS Parent Family/Friend Public Service Announcement (tv, radio) Agency Referral Mailings Other
No Secondary Caregiver (skip application for secondary caregiver) Secondary Caregiver General Information First Name M. Init. Last Name Gender Male Female B-Day English English Middle-Eastern Languages Middle-Eastern Languages Spanish Spanish Language Other Language Pacific Island Languages Pacific Island Languages Other __________________ Other __________________ Race Ethnicity White Bi/Multi-racial Unspecified Asian Black Other____________ Hispanic Native American Pacific Islander Bachelor or Advanced Degree Employed full time Some College/Vocational/ Homemaker Associates Degree Employed part time High School Graduate Retired or disabled Education Level Employment Status GED Job training or in school Grade 11 Employed seasonal Grade 10 Self employed Grade 9 or less Unemployed Education Completion Date (Active) Member of Employer / School Name US Military Veteran of US Military Phone Home: Mobile: Work: E-mail: Same as Primary Caregiver's Home Address City State Zip Code Medical Insurance Yes No Specify: Comments Primary: Secondary:
Child Information Agency Applicant For Current Year Next Year Center 1 Center 2 Center 3 Desired Center First Name Mid. Init. Last Name App. Date Gender Male Female B-Day Demographic Information English English Middle-Eastern Languages Middle-Eastern Languages Spanish Spanish Language Other Language Pacific Island Languages Pacific Island Languages Other __________________ Other __________________ Race Ethnicity White Bi/Multi-racial Unspecified Asian Black Other____________ Hispanic Native American Pacific Islander US Citizen Yes No Eligibility Information Parental Status (Check all that apply) Grandparent Teen Parent Student Parent Guardian Group Home Dual Custody Homeless Disabled Parent Foster Parent Relation to Primary Caregiver Relation to Secondary Caregiver Special Need Disability Status No Suspected Certified IEP Certified IFSP Child Protective Services Death of Immediate Family Member (Within the previous 12 months) Non-English Speaking Part Day, 4 days per week Desired Program Option Full Day, 4 days per week Full Day, 5 days per week
Additional Information Family Size In order to help establish program eligibility, we must determine the size of your family using the definition of "family" found in 45 CFR Part 1305.2(e) of the Head Start Program Performance Standards. This definition states that family means "all persons living in the same household who are: (1) Supported by the income of the parent(s) or guardian(s) of the child enrolling or participating in the program, AND (2) related to the parent(s) or guardian(s) by blood, marriage, or adoption OR (3) the child’s authorized caregiver or legally responsible party. Name Male Female D.O.B. Relation to Child Name Male Female D.O.B. Relation to Child Name Male Female D.O.B. Relation to Child Name Male Female D.O.B. Relation to Child Name Male Female D.O.B. Relation to Child Total # of family members (including child & caregivers) Transportation Yes No Will you need Head Start to transport your child to and from school each day? Please give directions to your home (be very specific) Emergency Information Name Yes No Release to: Emergency Contact: Yes No Phone # Name Release to: Yes No Emergency Contact: Yes No Phone # Yes No Name Release to: Emergency Contact: Yes No Phone # Name Release to: Yes No Emergency Contact: Yes No Phone # I authorize the above designated persons to be contacted in case of emergencies and/or for release of my child. I certify that all information that I have provided in this application is complete and correct. I understand that if I knowingly provided false information, participation in this agency's program may be terminated and my family may not be eligible for further services. I also understand that the information provided will be kept confidential. Back to Presentation Parent / Guardian Signature Date Staff Signature Title / Position
#3
Back to Presentation
Change of Status Please use this form to record necessary changes made during the year to the original child and family information listed on the application. This sheet should then be attached to the application. The parent is only required to sign this form if he/she is making a change in the Emergency Contact Information section. Child Name Classroom Teacher Center General Information Legal Name Change For: Child (Check One) Change From: Parent Change To: Change of Address / Phone: Type New Address: New Phone #(s): Identify if phone # is home, work, or cell in "type" space Transportation: Pick up location: Drop off location: Directions to Home: Emergency Contact Information Emergency Contact Information Change of Insurance: Child Primary Caregiver Please use the sections below and the corresponding boxes to add or delete individuals (from the orginal list given by the parent) that a child may be released Please use the sections below and the corresponding boxes to add or delete individuals (from the orginal list given by the parent) that a child may be released Secondary Caregiver Previous Insurance to or may be contacted in case of an emergency. You will also use this section to change phone numbers for emergency contacts. If the person will not to or may be contacted in case of an emergency. New Insurance be an emergency contact, the phone # is not required. Emergency Contact Information Release To Contact Please use the sections below and the corresponding boxes to add or delete individuals (from the orginal list given by the parent) that a child may be released Release To Contact to or may be contacted in case of an emergency. You will also use this section to change phone numbers for emergency contacts. If the person will not be an emergency contact, the phone # is not required. Yes No Yes No Name: Release To Contact Yes No Yes No Name: Phone: Yes No Yes No Name: Phone: Yes No Yes No Yes No Yes No Name: Name: Phone: Yes No Yes No Name: Phone: Parent/Guardian Signature: Parental Status This section should only be used if the child has been placed with a new family Parent/Guardian Signature: Parent/Guardian Signature: Parental Status has now changed to the following: Biological Parents Foster Care Other List information for the new caregivers: PC Name SC Name D.O.B. D.O.B. Gender Gender Education Level Education Level Employment Status Employment Status Employer Name Employer Name Comments If you have any additional comments concerning a change in this child's information, please list them on the lines below: Staff Signature Date
Only the parent/stepparent/guardian can fill out an application for a child to enroll in Head Start and only their income can be used. A person with educational rights for the child can do parent conferences, sign field trip permission, or other documents that relate to the child’s education but the person cannot provide the information that leads to the child’s eligibility. Back to Presentation
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries