This training will begin at 12:00pm ET WebEx Technical Support: 1-866-229-3239 Or e-mail us at nationalhivcenter@fenwayhealth.org
Works with HIV/AIDS service organizations and community-based organizations to navigate the changing health care landscape Goals: • Improve organizational sustainability and effectiveness for ASOs/CBOs • Improve care along the HIV continuum (the treatment cascade) Methods • Webinars, learning tools, issue briefs • Individualized technical assistance for Ryan White-funded ASOs/CBOs
The Fenway In Institute Research, education, & health policy Fenway Health A federally qualified health center with 25,000 patients, about 10% of whom are living with HIV Ryan White Part C provider: Largest provider of HIV care in New England
AIDS United works to end the AIDS epidemic in the U.S. through strategic grant making, capacity building, policy advocacy, technical assistance, and formative research. (Aids United Homepage) ARCW is home to the ARCW Medical Center, which provides integrated care and services to more than 3,000 people living with HIV through its CMS approved Medical Home. ARCW has provided training and TA to ASOs in 22 states. (ARCW Homepage)
Conta tact t us with ith any y questi tions about th the Cente ter or to get added to our maili iling lis list! 617.927.6028 nationalhivcenter@fenwayhealth.org www.nationalhivcenter.org
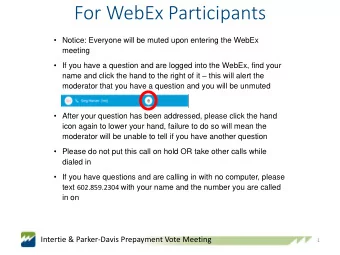
Please call WebEx Technical Support: • 1-866-229-3239 You can also contact the webinar host, using the Q&A panel in the right hand part of your screen. To see the panel, you may need to expand the panel by clicking on the small triangle next to “Q&A” Alternatively, e-mail us at nationalhivcenter@fenwayhealth.org
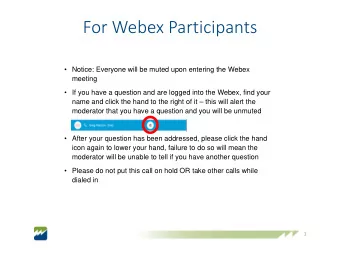
Check if your computer speakers are muted If you are unable to listen through your computer speakers: • Click on the “Info” tab at the top of the screen • Pick up your telephone, and dial the phone number and access code.
When the webinar concludes, an evaluation will automatically open for you to complete We very much appreciate receiving feedback from all participants Your feedback will help inform our program and plan our upcoming webinar curriculum
Download copies of today’s slides from our website: National HIV Center Homepage Today’s presentation will also be archived and available to view on-demand within a week. For this archived webinar, as well as all of our previous webinars, please visit the webinar section of our website: National HIV Center Homepage
Gr Greg Do Doggett
Greg g Doggett, JD JD, , CAE Counsel, Legal and Poli licy Affair irs 340B Health th Th Thursday, Ju June 16, , 2016 1:0 :00 - 2:0 :00 PM EDT
This presentation is not to be construed or relied upon as legal advice.
Program Overview Key Program Requirements Audits & Recertification Legislative Developments Regulatory Developments Resources
340B Program Overview
Nonprofit association that represents over 1,200 hospitals in the 340B program – all hospital types At the table since inception of program in 1992 The only advocacy organization focusing exclusively on 340B hospitals Provides technical assistance on 340B issues
Program created in 1992 to give safety-net providers discounts on outpatient drugs Administered by the Office of Pharmacy Affairs (OPA) within the Health Resources and Services Administration (HRSA) In order to have their drugs reimbursed by Medicaid and Medicare Part B, manufacturers must participate in the 340B program by entering a Pharmaceutical Pricing Agreement with the federal government Program purpose: To help eligible safety net providers “stretch scarce Federal Resources as far as possible, reaching more eligible patients and providing more comprehensive services.” • Source: H.R. Rep. No. 102-384(II), at 12 (1992).
Provide drugs or services for free or at reduced cost to patients who cannot afford them Drugs provided at market rates to insured patients, generating funds that providers use to improve and expand patient care
Ryan Whit ite HIV IV/AIDS Program Grantees Hosp spit itals ls • Disproportionate Share Hospitals • Critical Access Hospitals • Sole Community Hospitals • Rural Referral Centers • Freestanding Children’s Hospitals • Freestanding Cancer Hospitals
Hea ealt lth Cen enters • Federally Qualified Health Centers (FQHC) • FQHC Look-Alikes • Native Hawaiian Health Centers • Tribal/Urban Indian Health Centers Spe pecializ ized Clin inics • Black Lung Clinics • Hemophilia Treatment Centers • Title X Family Planning Clinics • Sexually Transmitted Disease Clinics • Tuberculosis Clinics
According to the HRSA website, the 340B program covers the following outpatient drugs: • FDA-approved prescription drugs; • Over-the-counter (OTC) drugs written on a prescription; • Biological products that can be dispensed only by a prescription (other than vaccines); or • FDA-approved insulin
Brand-name drugs (except clotting factor and drugs approved exclusively for pediatric use) • Generally, 340B price is average manufacturer price (AMP) – 23.1% of AMP • AMP: The average price paid to manufacturers by wholesalers for drugs distributed to retail community pharmacies and retail community pharmacies that purchase drugs directly from manufacturers. • Additional discount if best price is lower or price increased more quickly than rate of inflation • Best price: The lowest price paid to a manufacturer for a brand name drug, taking into account rebates, chargebacks, discounts, or other pricing adjustments, excluding nominal prices
Generic drugs & prescription OTC drugs: AMP – 13% of AMP • October 2015: Congress passed legislation that will require manufacturers to provide greater discount if price of generic drug increased more quickly than rate of inflation • Goes into effect January 1, 2017 Clotting factor and drugs approved exclusively for pediatric use: AMP – 17.1% of AMP
Key Program Requirements
Key legal/compliance requirements for 340B program: • 340B Eligibility • Eligible Patients/Patient Definition (e.g., generally any insured or uninsured outpatients of provider) • Medicaid & 340B/Duplicate Discount Prohibition • Contract Pharmacy This presentation focuses on legal/compliance requirements as they exist today • The mega-guidance, released by HRSA in August 2015, proposed significant changes to the types of patients that can use 340B, but has not been finalized • Could substantially reduce the number of patients eligible to receive 340B drugs HRSA evaluates compliance through selective audits of covered entities (CEs) and annual recertification Policies and procedures in these program areas (and others) are critical!
Entities are not eligible for the program unless they register and are listed on the OPA database If there is a change in a Covered Entity (CE)’s eligibility status, the CE has a responsibility to immediately notify OPA and should stop purchasing drugs through the 340B program CEs must recertify their eligibility every year and attest to ongoing compliance with key program requirements
Eligible Patients: Patients who are eligible to receive 340B drugs Diversion: Provision of 340B drugs to ineligible patients The 340B statute requires CEs to avoid committing diversion How does a CE avoid diversion? Create and follow policies and procedures that: • Describe how you make sure 340B drugs are not given to ineligible patients • More complicated for some providers than others • If applicable, explain the circumstances under which a patient is 340B- eligible when a script is written offsite (e.g., documenting referrals) • Describe process for inventory management • Describe how you conduct self-audits to ensure diversion is not occurring
HRSA’s 1996 guidelines (61 Fed. Reg. 55156 (Oct. 24, 1996)): • The covered entity has established a relationship with the individual, such that the covered entity maintains records of the individual’s care; and • The individual receives health care services from a health care professional who is either employed by the covered entity or provides health care under contractual or other arrangements (e.g., referral for consultation) such that responsibility for the care provided remains with the covered entity; and • The individual receives a health care service or range of services from the covered entity which is consistent with the service or range of services for which grant funding or Federally-qualified health center look-alike status has been provided to the entity. • Third part applies to HRSA grantees only and not to hospitals
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries