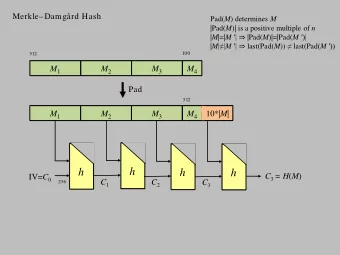
4/15/2016 • No relevant disclosures The Work Up of PAD in the Young – Be Careful (Likely Not PAD) David Rigberg, MD Professor of Surgery UCLA/DGSOM Vascular Disease in Young Adults Causes • Accelerated Atherosclerosis • Not common, but not rare -metabolic or clotting abnormality* • Easy to assess, so don’t overlook -radiation • Trauma • Frequently have palpable pulses, so • Thromboangiitis obliterans provocation needed • Coarctation • Can be associated with other conditions or • Vasculitis stand alone process • Premature popliteal aneurysm • Persistent Sciatic Artery *22 percent mortality at 5-10 years of claudication intervention 1
4/15/2016 Chronic exertional compartment Causes syndrome -young runners • Chronic exertional compartment syndrome -usually bilateral • Popliteal Entrapment -need ICP measurements to confirm • Adventitial Popliteal Cystic Disease Pedowitz criteria • Iliac Endofibrosis 1. Resting ICP > 15 mm Hg 2. ICP > 30 mm Hg 3 min S/P exercise 3. ICP > 20 mm Hg 5 min S/P exercise -Usually treated with open fasciotomy (-ectomy) Popliteal Entrapment Etiology • Common in young pts with claudication (60 %) • Embryologic • Active patient (“jogging disease”) • Development of medial head gastroc • Most pts < 30 • Should come from post fibula and lat tibia • Most pts male • Attaches to post medial fem condyle • Up to 2/3 with some anatomic problem b/l 2
4/15/2016 Classification Type I: artery completes development before migration. Normal muscle insertion Type II: abnormal insertion of muscle Type III: abnormal muscle slip Type IV: persistence of embryologic artery Type V: add the vein Type VI: functional. Muscle be more medial Presentation • Usually claudication • Acute ischemia rare • Can have findings of tibial nerve or pop vein • Palp pedal pulses; decrease with passive DF or active PF (tense the Gastroc) • Distal emboli can occur • Can be thrombosed at presentation 3
4/15/2016 Diagnosis • H & P suggestive • Noninvasive lab – exercise ABI or PDF/APF • CTA • MRA • Angio – rarely. Good to assess runoff if poor Treatment • Musculotendon release • Can divide medial head of gastroc for I-II • Types III-IV need muscle of medial head off posterior condyle • If artery is compromised, reconstuct • GSV/SSV • Type IV usually take muscular head (not tendon) 4
4/15/2016 Accessory slip Adventitial Cystic Disease • 1/1200 claudicants • Cyst takes up lumen of vessel; functional stenosis • Occlusion can occur • Can occur throughout the body • Can occur in veins as well Ogino, et al The etiology and management of cystic adventitial disease NM. Desy, R J. Spinner Journal of Vascular Surgery, Vol. 60, Issue 1, p235–245.e11 Etiology • Synovial theory: -synovium breaches articular space -involves adventitia of adjacent vessel -analogous to synovial or ganglion cyst 5
4/15/2016 Diagnosis • H & P • Typically have palpable pulses -diminished pulse with flexion of knee (Ishikawa’s sign) • Imaging shows eccentric stenosis: “Scimitmar Sign 6
4/15/2016 Treatment • Cyst drainage -recur -doesn’t necessarily restore artery • Removal of cyst from artery -not a clean plane -leaves damaged artery -tend to recur • Excision of cyst (and articular branch?) -usually replace with GSV graft 7
4/15/2016 Iliac Endofibrosis • Usually high performance cyclists • Normal pulses (if artery open) • Can be tolerant to high degree • Tortuosity and kinking can occur • Process involves intimal thickening Diagnosis • H & P • Normal pulses unless thrombosed or embolization • Provocative Testing -May need to bring in cycle -Positioning for CTA (protocols) 8
4/15/2016 9
4/15/2016 10
4/15/2016 Treatment • RP exposure – one side at a time -muscle sparing -pts anxious to get back to cycling • Usually patch angioplasty • May need to shorten artery • May need to perform thrombectomy • Occasionally need bypass Conclusions • Vasc Disease in younger patients is not rare • Provocative testing frequently needed! • Younger patients with bigger performance demands • Excellent results can be obtained for most of the non-atherosclerotic pathologies 11
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries