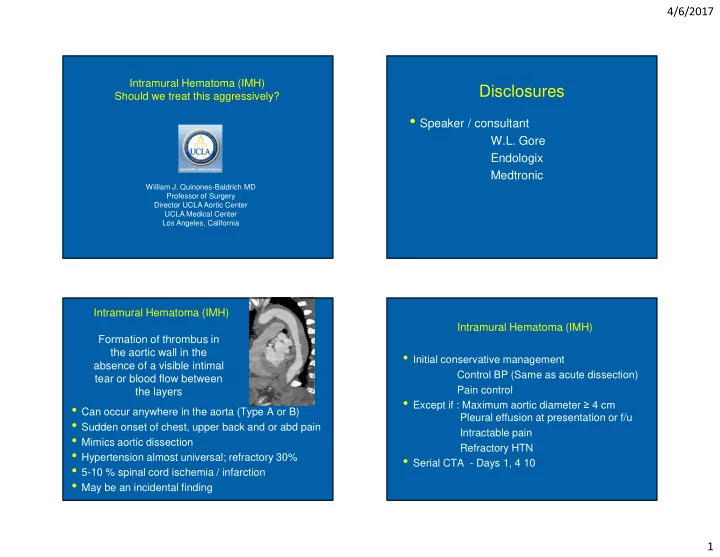
4/6/2017 Intramural Hematoma (IMH) Disclosures Should we treat this aggressively? • Speaker / consultant W.L. Gore Endologix Medtronic William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles, California Intramural Hematoma (IMH) Intramural Hematoma (IMH) Formation of thrombus in the aortic wall in the • Initial conservative management absence of a visible intimal Control BP (Same as acute dissection) tear or blood flow between Pain control the layers • Except if : Maximum aortic diameter ≥ 4 cm • Can occur anywhere in the aorta (Type A or B) Pleural effusion at presentation or f/u • Sudden onset of chest, upper back and or abd pain Intractable pain • Mimics aortic dissection Refractory HTN • Hypertension almost universal; refractory 30% • Serial CTA - Days 1, 4 10 • 5-10 % spinal cord ischemia / infarction • May be an incidental finding 1
4/6/2017 Intramural blood pool Intramural Hematoma (IMH) Ulcer like projection (ULP) vs Penetrating aortic ulcer (PAU) Areas of focal contrast enhancement ULP vs PAU(atherosclerosis) within the intramural hematoma without lumen communication Intramural Hematoma (IMH) vs TBAD IMH Follow up Conservative Management Partially healed type B Aortic Dissection? 2014 Initial presentation 6 weeks later Spontaneous false lumen thrombosis (4%) 2
4/6/2017 Intramural Hematoma (IMH) vs TBAD Intramural Hematoma (IMH) vs TBAD Follow up Conservative Management Follow up Conservative Management 2015 2016 Intramural Hematoma (IMH) vs TBAD Follow up Conservative Management Feb 2017 IRAD registry: IMH 107 patients vs ATBD 790 patients Most IMHB patients can be treated medically, and aortic enlargement is less common during follow- up, which may suggest that IMHB may have a slightly more benign course compared with classic ABAD in the acute setting. J Vasc Surg 2013;58:1498-504 3
4/6/2017 Intramural Hematoma (IMH) Indications for TEVAR on follow up • Increase in IMH thickness • Extension of IMH • New Ulcer Like Projection (ULP) • New aortic wall “pool” • Intractable pain • Refractory HTN J Vasc Surg 2016;64:1569-79 Intramural Hematoma (IMH) Intramural Hematoma (IMH) TEVAR considerations Conclusions • Do not exceed 10% oversizing • May be a continuum of medial aortic pathology • Cover all affected aorta; if not possible be aware • Conservative management is first line of therapy new tear with dissection / extension can occur • TEVAR for specific acute or subacute indications • Proximal landing zone on “healthy” normal • Close follow up indicated in all cases appearing aorta • TEVAR is intervention of choice with specific • Avoid ballooning considerations • Retrograde dissection is a risk – avoid bare metal • Need for open repair very rare proximal stent configuration 4
4/6/2017 UCLA Aortic Center Thank you aorticcenter.ucla.edu 310-AORTAFIX (310-267-8234) 5
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries