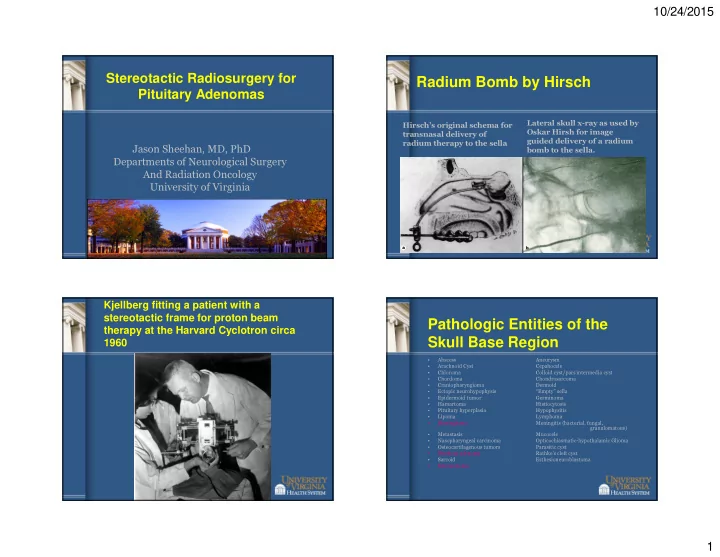
10/24/2015 Stereotactic Radiosurgery for Radium Bomb by Hirsch Pituitary Adenomas Lateral skull x-ray as used by Hirsch’s original schema for Oskar Hirsh for image transnasal delivery of guided delivery of a radium radium therapy to the sella Jason Sheehan, MD, PhD bomb to the sella. Departments of Neurological Surgery And Radiation Oncology University of Virginia Kjellberg fitting a patient with a stereotactic frame for proton beam Pathologic Entities of the therapy at the Harvard Cyclotron circa Skull Base Region 1960 • Abscess Aneurysm • Arachnoid Cyst Cepahocele • Chloroma Colloid cyst/pars intermedia cyst • Chordoma Chondrosarcoma • Craniopharyngioma Dermoid • Ectopic neurohypophysis “Empty” sella • Epidermoid tumor Germinoma • Hamartoma Histiocytosis • Pituitary hyperplasia Hypophysitis • Lipoma Lymphoma • Meningioma Meningitis (bacterial, fungal, granulomatous) • Metastasis Mucocele • Nasopharyngeal carcinoma Opticochiasmatic-hypothalamic Glioma • Osteocartilagenous tumors Parasitic cyst • Pituitary adenoma Rathke’s cleft cyst • Sarcoid Esthesioneuroblastoma • Schwannoma 1
10/24/2015 Stereotactic Neuro- Indications for GKS Imaging Techniques CISS • Thin cut (1 mm), post- contrast axial and coronal • Recurrent or residual adenomas – Persistence of hypersecretory state in MRI’s through the region those with functioning pituitary adenomas of the tumor and the skull – High incidence of recurrence in those base. with – Fat suppression MRI protocols in post-op patients • Cavernous sinus invasion – Oldfield – Dynamic MRI • Dural invasion – Wrightson; Laws – T2 or CISS sequences • Silent ACTH, GH, or TSH staining • Dynamic MR Dynamic MRI • As a primary treatment – Rapid scanning with fast GRE – When comorbidities prevent extirpation sequence during contrast infusion to increase detection of – When there is no need for urgent microadenomas decompression of the optic apparatus – 10 second sequence is repeated – Typically need at least 2 mm of clearance up to ~2 minutes between the optic apparatus and the • CT scans adenoma to deliver an effective dose to – Less distortion the whole tumor – Useful for dose planning – When there is clear radiological and calcuations endocrinological evidence of a pituitary adenoma Cav Sinus Invasion POSTCONTRAST MPRAGE POSTCONTRAST MPRAGE WITH WITHOUT FAT SUPPRESSION FAT SUPPRESSION 0 Radiologic Control 1 2 • Most series show >90% control of adenomas. 3a • Higher doses required for functioning adenomas (18-30Gy) 3b 4 2
10/24/2015 Nonfunctioning Adenomas Early vs. Late GKRS Average Tumor Control 95.7% GKRS within 6 months Matched cohort NFA Assessed for TSR Residual patients • Tumor control Adenoma • Hypopituitarism • Need for additional tx GKRS > 6 months Extent and Time to Endocrinopathy rates after GKRS in NFA patients in the early and late cohorts Endocrine Remission 1 Cushings • Endocrine remission in Endocrinopathy rate (% of cohort) approximately 50-70% of patients Median time to remission • Times to achieve endocrine On ketoconazole=21.8 months 0.8 remission vary – Cushing’s—fast Off ketoconazole=12.6 months P=0.036 – Acromegaly---moderate P=0.012 – Nelson’s and Prolactinomas—slow – However, appears faster than with 0.6 Early SRS of residual NFA may avoid endocrinopathy standard external beam radiotherapy • We improve extent of remission (as well as tumor growth) Early (n=32) with 0.4 – Higher dose (>25Gy) Acromegaly – Smaller treatment volume Late (n=32) – Better targeting – Cessation of antisecretory 0.2 medications 0 0 20 40 60 80 100 Endocrine follow-up after GKRS (months) 3
10/24/2015 SRS for Cushing’s Disease SRS for Acromegaly Mean remission 45-50% in 1-2 years Mean remission 50% in 1-2 years Example of Acromegalic Pt Effect of Antisecretory 36y/o woman with persistent acromegaly 9/2007 and 8/2008 TSR’s for pituitary macroadenoma Medications 12/2008- GKRS SRS: 25Gy, 50% 7/2009 9/2007 10/2008 7/2012 • Antisecretory medications appear to be radioprotective – However, thus far, only single center, retrospective studies • Period of cessation depends upon the GH 16.29999924 16.79999924 Endocrine Suppression 20 14.89999962 11.60000038 pharmacology of the 1.0 6.099999905 10 3.799999952 agent Cumulative Probability of Not Yet Being Cured 0.9 Endocrine Suppression No 0 0.8 TSS Yes - - - - - - - - • However, most patients 0.7 TSS GKS Sandostatin can tolerate a period of 6- 0.6 Sandostatin Remission 0.5 8 weeks off suppressive 0.4 at 38 months medications 0.3 0.2 0.1 0.0 0 10 20 30 40 50 60 70 80 90 100 110 120 Time to Cure (months) 4
10/24/2015 Delayed Hypopituitarism Radiation Sensitive Structures • Well respected groups have • However, not likely reported a low incidence (0- that simple. 52%) of pituitary dysfunction • Likely related to dose following radiosurgery. per volume of • Dysfunction may occur >10 structure. years following radiosurgery. • Hypopituitarism has been • Dose restriction to a reported in patients following functioning adenoma doses of less than 10Gy to the is not warranted. pituitary gland. • Must strive for • There may be no completely safe dose to deliver to the endocrine remission. normal gland, hypothalamus, • Hypopituitarism can or stalk be medically managed. • The actuarial risk of delayed Radiosensitivity hypopituitarism increases even 10 years after SRS Stalk (6 Gy)>Gland>Median Eminence>Hypothalamus Source: Feigl et al., JNS Suppl (2005) Spacer between normal gland Timing of New Endocrinopathies and Adenoma • Couldwell and colleagues describe 34 patients – Median f/u of 4 years – 47% FSRT; 53% SRS Hypopituitarism Pituitary gland – Limited dose to normal gland tumor % with new to 12 Gy or less 30% at 5 years – No delayed endocrinopathies endocrinopathy – 18% tumor recurrence or 50% at 10 years progression at • May lessen the risk of Hypopituitarism Taussky et al., JNS, 2011 Xu, Neurosurgery, 2013 Months after radiosurgery 5
10/24/2015 1.5T 3T Improvement with Advances in Hypopituitarism at UVA Neuro-Imaging • What techniques will New Endocrinopathy improve outcomes? – 3T imaging • Better target definition Thyroid - 20.8% • Improved visualization of IGF-1 - 16.7% critical structures Cortisol-8% • Frame Distortion Gonadotropin 4.2% • Co-registration Diabetes Insipidus - 2% – Higher 5T and greater None 61% – PET imaging – Tractography Optic Neuropathy after Radiosurgery Optic Nerve Injury • Mayo, 2003 -- "A study on the radiation • Graz, 1998 (Austria) -- "Dose-response • The optic apparatus tolerance of the optic nerves and chiasm after tolerance of the visual pathways and cranial stereotactic radiosurgery." (Stafford SL, Int J nerves of the cavernous sinus to stereotactic is the most sensitive Radiat Oncol Biol Phys. 2003 Apr 1;55(5):1177- radiosurgery." (Leber KA, J Neurosurg. 1998 81.) Jan;88(1):43-50.) – Retrospective. 218 Gamma Knife plans (122 – Retrospective. 50 patients with gamma knife of the cranial nerves sellar/parasellar, 89 pituitary, 7 treatment of middle cranial fossa. Mean F/U 40 cranipharyngiomas). Prior RT in 11% patients. months Median F/U 40 months – Optic neuropathy: 0% if <10 Gy, 27% if 10-15 Gy, to radiation. – SRS: median max 10 Gy (0.4-16.0) 78% if >15 Gy – Radiation optic neuropathy: 4 patients (2%) at – Conclusion: 10 Gy maximum tolerable dose – Tolerable levels median 48 months. All had prior surgery, 3/4 • Pittsburgh/MGH, 1993 -- "Tolerance of prior EBRT (risk 0.5% vs. 13%). cranial nerves of the cavernous sinus to – Conclusion: Risk of RON 1% if "short" segment range from 8 to 14 dose <=12 Gy. "Long" segment to 9 Gy may radiosurgery." (Tishler RB, Int J Radiat Oncol carry a significant risk. Short vs. long not enough Biol Phys. 1993 Sep 30;27(2):215-21.) data to define Gy. – Retrospective. 62 patients with lesions around cavernous sinus. Treated with GKS (33 patients) • Maryland, 2000 -- "Preservation of visual or 6MV linac (29 patients). Median F/U 19 fields after peri-sellar gamma-knife months – Generally noted to radiosurgery." (Ove R, Int J Cancer. 2000 Dec – Optic complications: 4 patients, dose response 20;90(6):343-50.) seen (4/17 dose >8 Gy; 0/35 dose <8 Gy) be 1% volume or a – Retrospective. 20 patients, 90% pituitary – Conclusion: Dose to optic apparatus should be adenomas. Median F/U 24 months <8 Gy – SRS: mean max dose 9 Gy (2.5-14.1), volume maximum (i.e. point average of optic chiasm 5.2 Gy. – Complications: none dose) – Conclusion: 8 Gy conservative and 10 Gy justifiable Conclusion: Optic nerve & chiasm max. tolerable dose: conservatively 8 to 10 Gy; point dose 12 Gy Majority of optic neuropathies<2 years, but some can develop 3+ years later 6
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries