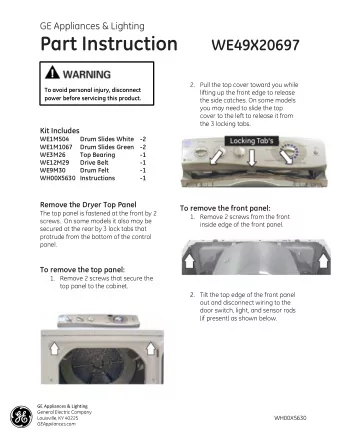
Practice Variability in the Management of Pediatric Pancreatic Trauma Bindi Naik-Mathuria, MD and members of the Pediatric Trauma Study Group Falcone R Burd R Puapong D Mooney D Campbell B Kreyekes N Fenton S Gourlay D Jacobs D Vogel A Gibbs D Hamner C Upperman J Beaudin M Kulp H Burke R Abdelssalam S Russell R Gosain A
Background • Non-operative management of other blunt solid organ injuries (spleen/liver/kidney) is now considered standard of care in pediatric trauma • The pancreas however, remains an organ of debate… Page 1 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:17 PM
AAST CT Grading Scale for Pancreatic Trauma Grade Type of Injury Description of Injury I Hematoma Minor contusion without duct injury Laceration Superficial laceration without Observation duct injury II Hematoma Major contusion without duct injury or tissue loss Laceration Major laceration without duct injury or tissue loss III Laceration Distal transection or parenchymal Observation? injury with duct injury Distal Pancreatectomy? IV Laceration Proximal transection or parenchymal injury involving Observation vs. ampulla Complex Operative Management V Laceration Massive disruption of pancreatic head Page 2 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:18 PM
Page 3 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:18 PM
EAST Trauma Management Guidelines (2009) • Level III evidence: • Grade I and II injuries can be managed by drainage alone • Grade III injuries should be managed with resection and drainage • “Management of pediatric injuries seems to follow many of the same principles as those for adults, albeit with key exceptions in the potential role for non- operative management .” Page 4 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:18 PM
Journal of … … Pediatric … Surgery … Volume 22, Issue 12, … December 1987, Pages … 1110-1116 » Blunt injury to the pancreas in children: Selective management based on ultrasound * 1 1 Arkadi Gorenstein , Dara O'Halpin , David E. , 1 1 1 Wesson , Alan Daneman , Robert M. Filler Toronto, Ontario, Canada Page 5 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:19 PM
NOM had more interventions Page 6 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:19 PM
Variable Clinical Management in NOM? • When to feed? • How to feed? • Pseudocyst management? • Role of ERCP? • Time on TPN • Length of hospital stay • Number of interventions Page 7 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:19 PM
Page 8 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:20 PM
PTS Pancreatic Trauma Study Group Page 9 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:20 PM
Purpose • To prove the hypothesis that practice variability exists among pediatric trauma surgeons regarding high-grade pancreatic injuries • Preference for OM or NOM • Clinical management of NOM • To assess feasibility of a prospective, randomized, controlled trial comparing outcomes of OM and NOM Page 10 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:21 PM
Method Page 11 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:21 PM
Results • Data collected from 19 centers • 123 injuries (> grade 1) 41 reported over the past 3 33 32 years • Median 6 per center 17 • Range 1-22 per center • 75 duct injury/suspected Grade II Grade III Grade IV Unclear/Unknown • Median 1 per center Pancreatic Injuries at 20 Pediatric Trauma Centers (3 years) • Range 0-8 per center Page 12 Surgical Services xxx00.#####.ppt 11/12/2015 12:46:21 PM
Results • 5 centers used NOM for all cases 59% • 2 centers used OM for all 41% NOM OM cases • 12 centers (63%) used both approaches 21% were laparoscopic Page 13 Surgical Services xxx00.#####.ppt 11/12/2015 12:46:22 PM
Clinical Management of NOM Cases “Which are the primary management strategies for non - operative patients used at your center?” 16 Yes No 14 12 10 50% 8 6 4 2 NPO until NPO until NPO until NPO until NPO until Early jejunal Early ERCP Percutaneous ERCP only if 0 labs normal labs normal pseudocyst amylase/lipase epigastric feeds with.without drain for pseudocyst A B C D E F G H I AND OR resolved normal tenderness stent pseudocyst develops tenderness tenderness improved improved improved Page 14 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:22 PM
Results • MRCP is available at 89% of centers • MRCP is considered standard of care at 68% of centers • ERCP is utilized by 73% of centers • 63% of centers are willing and 26% may be willing to randomize patients to either NOM or OM strategy Page 15 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:23 PM
Conclusions • Practice variability exists among pediatric surgeons regarding the management of high-grade pancreatic injuries • Most centers surveyed use both the NOM and OM approaches (equipoise) • NOM varies too widely to make meaningful retrospective comparisons of outcomes among centers • A prospective trial to compare outcomes is feasible Page 16 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:23 PM
Limitations • Population surveyed had already expressed interest in comparing outcomes of OM and NOM • Only pediatric trauma centers were surveyed Page 17 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:23 PM
Future Directions • Prospective, multicenter, controlled trial to compare outcomes of OM and NOM • Develop best practice management guidelines for NOM to limit variability bnaik@texaschildrens.org Page 18 Surgical Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:24 PM
Thank You! Page 19 Surgical Services Trauma Services Trauma Services xxx00.#####.ppt 11/12/2015 12:46:24 PM
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries