Objectives Update on Aneurysm and To understand evidence-based - PowerPoint PPT Presentation
Objectives Update on Aneurysm and To understand evidence-based recommendations for intracerebral aneurysm Subarachnoid Hemorrhage (IA) detection and screening. Nerissa U. Ko, MD, MAS To understand the evidence-based treatment UCSF
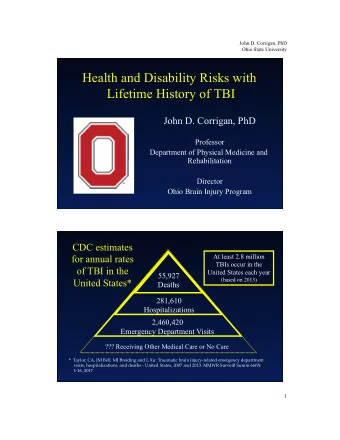
Objectives Update on Aneurysm and • To understand evidence-based recommendations for intracerebral aneurysm Subarachnoid Hemorrhage (IA) detection and screening. Nerissa U. Ko, MD, MAS • To understand the evidence-based treatment UCSF Department of Neurology algorithms for aneurysmal subarachnoid hemorrhage (SAH). September 6, 2014 Nothing to disclose Epidemiology Aneurysm Detection • Most detected incidentally by imaging • Prevalence of cerebral • Majority are asymptomatic, unruptured aneurysms is 3.6-6% (12 million in US) • Only 6% per year with symptoms • Majority are sporadically – Headache (focal or generalized) acquired lesions – Cranial nerves (dilated pupil, diplopia, vision loss, • An estimated 50-80% are dysarthria) small and unruptured – Brain stem (weakness, numbness,dizziness) • 20% of patients may have multiple aneurysms • Aneurysm rupture may be first symptom 1
Aneurysm Risk Factors Aneurysm Screening • General screening not recommended • Older age or cost-effective, but remains • More common in women controversial • Regional and ethnic differences • Exceptions in high risk genetic or rare familial conditions – Highest prevalence in Japan, Finland – Polycystic kidney disease, Ehlers-Danlos Type 4 – Blacks greater than whites – Family history of two first-degree relatives • Modifiable risk factors: HTN, tobacco, stimulants • Cerebral angiogram gold standard Immunodeficiency, excessive ETOH • Newer imaging modalities commonly • Associated with trauma (dissecting), infection used: CTA, MRA (mycotic), atherosclerosis, other vascular malformations (AVM) Lifetime Rupture Risk Genetics and Aneurysms • Familial studies have identified several loci • Candidate genes found potentially functionally active genes • GWAS further identified candidate genes, but difficult to replicate Korja M, et al. Stroke. 2014;45:1958-1963; Tromp G, et al. Annals of Medicine 2014; 1-10. Stijntje E Bor a, et al. Lancet Neurol 2014; 13: 385–92; Brown RD and Broderick J. Lancet Neurol 2014; 13: 393–404 2
Genome-wide microarray-based Genetics Syndromes Gene expression studies mRNA and microRNA expression • Polycystic kidney disease • Provide unbiased information about • Ehlers-Danlos Type 4 molecular mechanisms • Neurofibromatosis Type I and the foundation for functional studies. • Marfan’s Syndrome • Identified 430 upregulated and 617 • Pseudoxanthoma elasticum downregulated genes • Fibromuscular dysplasia • Can be good candidates for molecular markers of rupture-prone IAs and therapeutic targets Nakaoka H, et al. Stroke. 2014;45:2239-2245. Neurofibromatosis Type I Ehlers-Danlos Type 4 • Occurs in 1:50,000-500,000 persons • Occurs in 1:3,000-5,000 persons • Results in joint hypermobility, fragile skin, easy bruising, • Begins at birth and gets progressively worse and scarring • Of the five types, type IV is the most common and lethal • Results in vessel stenosis, vessel rupture, from deficiency in type III collagen neurofibromas and the abnormal • Aneurysms associated with this condition tend to form on development of the muscles, bones and medium to large arteries. internal organs • Aneurysms tend to form in medium to large- sized arteries. 3
Marfan’s Syndrome Polycystic kidney disease • PKD1>PKD2 • Occurs in 1:10,000 to 20,000 persons – 10% risk of cerebral aneurysms • Aneurysms tend to be saccular, fusiform, or dissecting – Risk of SAH < 1%, cause of death in 20% of patients in the proximal intracranial carotid artery – 18% will have a positive family history of aneurysm • Results in elongation of the bones and abnormalities in • Common autosomal dominant heritable the cardiovascular system (the heart and blood disorder (1 in 400-1,000 persons) vessels) and the eyes. • Cysts in the kidneys, liver, pancreas, and spleen, and hernias in the groin. • Hypertension is common (found in 75%), contributing to aneurysm formation and rupture Acute evaluation • Life-threatening illness that warrants a high index of suspicion • Misdiagnosis of SAH occurred in as many as 64% of cases prior to 1985, and remains approximately 12% currently • Misdiagnosis is associated with a 4-fold higher likelihood of 1-year death or disability. Edlow JA. Neurocrit Care. 2005;2(2):99-109. 4
AHA recommendations for evaluation High volume centers • Treatment volume is an important • CT scanning for suspected SAH, and lumbar determinant of outcome for intracranial puncture for analysis of CSF is strongly aneurysms – higher volume (>60 cases per recommended when the CT scan is negative. year) equals lower mortality and better long- term outcomes • Selective cerebral angiography to document the presence and anatomic features of • High volume centers should have appropriate aneurysms is strongly recommended in specialty neurointensive care units, patients with documented SAH. neurointensivists, vascular neurosurgeons and interventional neuroradiologists to provide • MRA or CTA can serve as useful alternative the essential elements of care (Class II). Class I, Level of evidence B. Why does it matter? Figure 2: Neurologic Complications after SAH • Transfer from low Figure 1: Outcomes after SAH volume centers is only 15% Hydrocephalus In-hospital mortality 17% • High-volume Rebleeding Out-of-hospital mortality centers are under 20% Vasospasm 16% Dependent utilized <4.5% 33% Hyponatremia 17% Independent without • Transfer of Cognitive deficits patients may be 30% Independent with Cognitive deficits cost-effective 1 2 3 4 5 6 7 8 9 10 11 12 13 14 • Lack of Days awareness of Cross DT, et al. J Neurosurg. 2003;99(5):810-817. these benefits Johnston SC. Stroke. 2000;31(1):111-117. Berman MF, et al. Stroke. 2003;34(9):2200-2207. 5
Objectives Rebleeding Medical Management • Increased time to • Up to 14% of SAH treatment is associated patients may with increased rates of • Rebleeding experience re-bleeding preoperative re- bleeding within 2 hours of the • Delayed cerebral ischemia – 0 to 3 days, 5.7% initial hemorrhage • Hyponatremia and volume management – 4 to 6 days, 9.4% • Re-bleeding was more – 7 to 10 days, 12.7% • ICU care: Glucose, anemia, temperature common in those with a – 11 to 14 days, 13.9% systolic blood pressure – 15 to 32 days, 21.5% control and DVT prophylaxis >160mm Hg • Post-op re-bleeding did • Anti-fibrinolytic therapy not differ among time may reduce re-bleeding intervals (1.6% overall) Adams HP, Jr., et al. Arch Neurol. 1981;38(1):25-29; Ohkuma H, et al. Stroke. 2001;32(5):1176-1180; Kassell NF, et al. J Neurosurg. 1990;73(1):37-47. Antifibrinolytic therapy Preventing Rebleeding • Early aneurysm repair. • Avoid delayed or prolonged antifibrinolytic therapy • Surgical clipping or endovascular coiling is strongly recommended • Antifibrinolytic therapy is relatively to reduce the rate of rebleeding. contraindicated in patients with risk factors for thromboembolism • Blood pressure should be monitored and controlled to • Patients treated with antifibrinolytic balance the risk of strokes, therapy should have close screening hypertension-related re-bleeding, for deep venous thrombosis and maintenance of cerebral • Consider an early, short course of perfusion pressure antifibrinolytic therapy • Treat extreme hypertension (MAP • Antifibrinolytic therapy should be >110 mmHg) with an unsecured, discontinued 2 hours before planned recently ruptured aneurysm endovascular aneurysm ablation 6
Delayed Cerebral Ischemia (DCI) DCI Treatment (contd.) Nimodipine Pressors Volume Endovascular • Oral nimodipine (60 mg • Patients clinically suspected • The goal should be • The use of routine every 4 h) should be of DCI should undergo a maintaining euvolemia, prophylactic angioplasty is administered after SAH for trial of induced rather than attempting to not recommended a period of 21 days hypertension induce hypervolemia • Endovascular treatment • The value of other calcium • Choice of vasopressor • Consider a saline bolus to using intra-arterial antagonists, whether should be based on the increase CBF in areas of vasodilators and/or administered orally or other pharmacologic ischemia as a prelude to angioplasty may be intravenously, remains properties of the agents other interventions considered for vasospasm uncertain related DCI • Blood pressure • Hemodilution in an attempt • With hypotension, dosing augmentation should to improve rheology should • Rescue therapy for ischemic intervals should be progress in a stepwise not be undertaken except in symptoms that remain changed, or may be fashion with assessment of cases of erythrocythemia. refractory to medical discontinued. neurologic function treatment DCI Novel Treatment Statins • Drugs such as statins, sodium nitrite, • Patients on statins prior to presentation with dantrolene, cilostazol, eicosapentaenoic acid aneurysmal SAH should have their medication continued in the acute phase • Intracranial delivery of nimodipine or magnesium • Acute statin therapy in statin-naive patients remains controversial for reducing DCI and • Volume strategies with albumin, and target- poor outcomes after SAH directed volume goals • STASH trial did not detect any benefit in the use of simvastatin 40 mg for long-term or short-term outcome in patients Kirkpatrick PJ, et al. Lancet Neurol. 2014 Jul;13(7):666-75 7
Recommend



More recommend
Explore More Topics
Stay informed with curated content and fresh updates.