It is predicted that over the course of the next 20 years obesity will be the number Bariatric Surgery: one health problem throughout the world Successes and Pitfalls Bradley J. Needleman, MD & Dara Schuster, MD The Ohio State University Columbus, OH Objectives • Review the short term and long term successes of bar iatric surgery • Discuss the short term and long term complications of bariatric surgery • Describe the necessary medical follow-up, monitoring and treatment plans for patients that have undergone bariatric surgery • Recognize the need for comprehensive weight management before and after surgery has occurred. 1
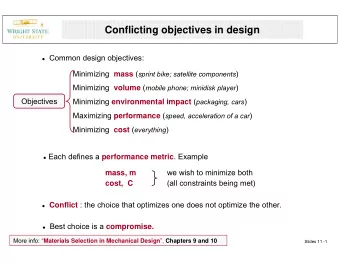
A Life-Threatening Relative Risks with Disease BMI>40 • Most studies show an increase in mortality rate associated with obesity (BMI > 30). Co-morbidities Men Women • Obese individuals have a 50% to 100% increased risk of death Breast CA 1.70 • When BMI > 45 Colon CA 1.84 1.36 � White men could lose up to 13 years of life Kidney CA 1.70 1.70 � White women up to 8 years of life. Liver CA 4.52 1.68 � African American men up to 20 years of life � African American women up to 5 years of life Bariatric Surgery Becomes Relative Risks with “Legitimate” BMI>40 • 1991 NIH Consensus Co-morbidities Men Women Developmental Conference Type 2 DM 10.65 19.89 � Medical weight loss unacceptably high incidence of weight regain after 2 years CAD 13.97 19.22 � Two treatments recommended as HTN 64.53 63.16 effective long term: • Roux-en-Y Gastric Bypass OSA 10.04 17.19 • Vertical Banded Gastroplasty 2
Bariatric Surgery Popularity of Bariatric Surgery Volume in U.S. • NIH- 1991 180000 160000 • Laparoscopy-1993 140000 120000 • Carnie Wilson 100000 80000 # of Operations • Al Roker 60000 40000 • ‘Patient Driven’ 20000 0 1993 1996 1999 2002 2005 • $$$$$$ ***16,800 operations in 1993 to 178,000 operations in 2005 Statistics on Weight Statistics on Loss Surgery Bariatric Surgeons • The number of gastric bypass surgeries climbed more than 600% from 1993 to 2003. • The number of active surgeons in the American Society for Bariatric • The average bariatric surgery patient Surgery jumped nearly 500 is a woman in her late 30s who weighs percent, from 168 in 1993 to 860 in approximately 300 pounds. 2003. • The average cost of the surgery is $30,000 3
Operations Performed The OSU Team in the U.S. • Surgeons • Restrictive (86%) • Dietitians � RYGBP (70%) • Psychologists � Lap-Band/VBG (16%) • PCRM’s and Nurse Practitioner • Exercise Physiologists • Malapsorptive (12%) � BPD � Duodenal switch • Medical Specialties Getting Patients to Bariatric Surgery at Surgery The OSU • Information Session and Application • 1976-Mason procedure • July 1977- 1st gastric stapling • Medical, Dietary and Psychological Evaluations and Labs/Testing procedure • 1979-Pace (single row TA-55) • Determination of Candidacy and Pre- Operative Requirements • 1982-Carey (silastic collar gastroplasty) � 4 weeks, 12 weeks, 6 months, 1 year • 1982-Martin (double row, liquid diet) � Education and behavioral modification 4
Bariatric Surgery at The Lap-Band The OSU • 1994- Open Gastric Bypass (TA-90B) • October 2000-Laparoscopic Gastric Bypass • February 2001- Lap Band (FDA C-trial) • April 2007- First U.S. Stomaphyx™ Postoperative The Roux-en-Y Gastric Bypass Management • Prevention of Cardiopulmonary • 15 - 30 cc pouch Complications • 12 -14 mm stoma � Sleep apnea, obesity hypoventilation syndrome • 75-150 cm Roux limb • DVT/PE prophylaxis (<2%) 5
Postoperative Impact of Volume on Management Outcomes � Morbidity • Monitoring for Surgical Complications • 28.0%, surgeons<10 cases/yr � Leaks (1%), Bleeding (2%), Dehiscence (Open) • 14.0%, surgeons high volume/yr • Antibiotics and Wound Care (p<0.05) • Ambulation and prevention of • Low volume hospitals 2.7 X pressure injuries increased risk of complications � Rhabdomyolysis versus high volume hospitals – Liu et al, Am Surg, 69:823-828, 2003 Impact of Volume on Laparoscopic Gastric Outcomes Bypass N OR Time LOS Follow-up Weight Loss • Surgeon volume for M&M in 4,685 cases in Pa – Courcoulas et al, Surgery,134:613-621 Wittgrove 500 120 min 2.6 60 73%EWL � Mortality • 5.0%, surgeons <10 cases/yr Higa 400 - 1.6 22 69%EWL • 0.3% surgeons high volume/yr, Schauer 275 247 min 2.6 30 77%EWL (100 cases, p=0.06) 6
Open Gastric Bypass Long-Term Concerns Series • Strictures • Cholelithiasis n Leak Hernia Followup Weight Loss Mortality • Marginal Ulcers • Hypoglycemia Sugerman 182 1.6% 18% 12 mo 67%EWL 1% • Kidney stones • Protein deficiencies Poires 608 - 23.9% 168 mo 49%EWL 1.5% • Eating disorders • Vitamin and Mineral deficiencies Capella 560 0 - 60 mo 62%EWL 0 • Addiction • Hernias Fobi 944 3.1% 4.7% 24 mo 80%EWL 0.4% • Maintenance of weight � port site and loss Maclean 243 - 16% 66 mo BMI44-29 0.41% internal hernias/sbo Weight Loss Curves Pouch Complications 100 • Strictures 80 � 5-20% and occurs b/w 3-8 weeks 60 BMI %EWL 40 � Treated with EGD and dilatation 20 0 Initial 6 mo 12 mo 18 mo 24 mo 30 mo Schauer et. al. 7
Small Bowel Pouch Complications Complications • Marginal Ulcer • Internal Hernias � 2-5% and can occur at any time � 3.3% incidence � NSAIDS, Smoking, Steroids, • 2/3 Petersen’s hernia Stress • 1/3 Mesenteric defect at � Treat with PPI’s, sucralfate Jejunojejunostomy � R/o Gastrogastric fistula • CT scan and UGI/SBFT neg. in >25% � Possible revision and vagotomy • May be emergency due to ischemia Small Bowel Stones Complications • Cholelithiasis • Incisional Hernias � Prophylactic vs. selective cholecystectomy � 15-20% in open cases, 1-2% in laparoscopy � 30% incidence of stones, 9% cholecystectomy � Decreases to ~1% w/ 6 months tx ursodiol 8
Definitions of Stones Success • Kidney stones • Weight loss � > 12 months post op � >50% EBWL � Increased serum oxalate-a and • Resolution of Co-morbidities decreased urine citrate � Diabetes, HTN, Sleep Apnea, Joint pains, Dyslipidemias, Venous Stasis, GERD • Patient Satisfaction Weight Regain- Psychiatry Failure • Coping/Depression/Divorce • Eating disorders • Weight regain at 10 years post-op � Anorexia � There was a significant ( P < 0.0001) � Bulemia increase in BMI in both morbidly obese (BMI < 50 kg/m2) and super obese • Addiction patients (BMI > 50 kg/m2) from the nadir to 5 years and from 5 to 10 years. � Alcohol � Sex Nicolas V. Christou, MD, Annals of Surgery, 11/2006 9
Weight Regain- Failure Novel Techniques in � There was a significant increase in failures and decrease in excellent the Treatment of results at 10 years when compared with 5 years. Obesity � The failure rate when all patients are followed for at least 10 years was 20.4% for morbidly obese patients and 34.9% for super obese patients. Nicolas V. Christou, MD, Annals of Surgery, 11/2006 Bridge Operations- Revision Surgery? Sleeve Gastrectomy • No data to determine who “best” and “worst” candidates for revisions • Can be performed as bridge to Gastric • Higher risk than original operation Bypass, Duodenal • Limited data on successes after revision Switch or Lap Band • Can be its own • Convert to gastric bypass weight loss operation • Revise pouch and anastomosis • Covert to “long-limb” bypass • ~57% EBWL @ 3 yrs • “Band” the bypass 10
BioEnterics Intragastric Endolumenal Sleeves Balloon (BIB): Development and testing of an attachable gastric cuff and small intestinal exclusion sleeve as a new flexible endoscopic method for treatment of obesity. Mitchell Dann, Josh Butters, Mary Lynn Wilmore, Dick Thomas, Tom Baldwin, Clay Robinson, Ray Olsen, Paul Swain St Mary’s Hospital and Imperial College, London, ValenTx, Inc. Wilson, Wyoming USA Endoscopic Restrictive Considerations Before and Gastroplasty After Surgery: Medical Sequelae of Obesity Dr. Ram Chuttani � Hypertension • ndo Plicator � Lipid disorders • ePTFE pledgets and pre tied suture � Diabetes • 4 pleats are formed � Ischaemic heart disease • Pleats are then � Cardiomyopathy joined to form ring � Pulmonary hypertension 11
Considerations Before and Considerations Before and After Surgery: Medical After Surgery: Medical Sequelae of Obesity Sequelae of Obesity � Immobility � Asthma � Breast/bowel/prostate/endometrial � Obstructive sleep apnea cancer � Gallstones � Venous stasis ulcers � NASH (Non-alcoholic steatohepatitis) � Intertrigo � Accident prone � Urinary incontinence Co-Morbidities in Considerations Before and After Surgery: Medical Bariatric Patients Sequelae of Obesity The OSU Experience � GERD 50 50 Peds % Adults % 45 45 � Arthritis/back pain 40 40 35 35 � Infertility/menstrual problems 30 30 25 25 � Obstetric complications 20 20 15 15 � DVT and thromboembolism 10 10 5 5 � Depression 0 0 OSA DM HTN OSA DM HTN 12
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries