Motility Disorders ESPGHAN Cape Town 2012 Jan Taminiau-Marc Benninga Academic Medical Center Amsterdam
How much can a person endure?
Patient with chronic intestinal pseudo- obstruction syndrome � 1 th day post partum: urine retention � 1 th year: recurrent UTI’s / constipation � Profylaxis AB / lactulose � 6 th year: Protuding abdomen � X-Abd: extremely distended bowel loops � Rectum suction biopsy (-) � Antroduodenale manometry (+) � Picture compatible with myopathy
Differential diagnosis Motility problem � Functional � Organic � Spinal abnormalities � Anorectal abnormalities � Endocrine � Cystic fybrosis � Medication � Munchhausen by proxy � Pseudo-obstruction � ????
Hirschsprung’s Disease Diagnostics?
Anorectal manometry rectal balloon IAS EAS side hole sleeve
Anorectal manometry IAS EAS side hole sleeve sleeve
Anorectal catheter neonates
Rectoanal inhibitory reflex in a premature (29wks) air insufflation anal sphincter (sleeve) mmHg 10 sec 30 J Pediatr 2001;139:233-5 J Pediatr 2003;143:603-5
Rectoanal inhibition reflex in a premature (29wks) air insufflation rectum anal sphincter anal sphincter anal sphincter 30 mmHg (sleeve) 10 sec
4 month old neonate with Hirschsprung’s disease air insufflation rectum anal sphincter anal sphincter anal sphincter 40 mmHg anal sphincter (sleeve) 10 sec
Anorectal manometry • The accuracy for the exclusion of Hirschsprung’s by manometry varies with the age of the patients • More accurate in older children, where studies have suggested an accuracy of 90-100% • Accuracy in neonates is lower (30 to 90%)
Caliber leap
Rectal suction biopsy Increased and thickened neurites Normal ACE staining
Chronic intestinal pseudo-obstruction Classification • Pathophysiological criteria − neuropathic CIP − myopathic CIP − unclassified (ICC’s ???) • Etiological criteria − congenital / familial − acquired (systemic diseases, post- infectious (CMV, EBV, HSV, polyomaviruses (JC virus) , drug- induced, ….)
CIPS Classification Type Myopathic Neuropathic Scleroderma, amyloidosis Early scleroderma, amyloidosis Infiltrative Myotonic and other dystrophies, Diabetes, porphyria, brain-stem tumor, Neurologic mitochondrial myopathy MS, spinal cord transsection, disease (MNGIE) dysautonomias (Shy-Drager) Paraneoplastic (small cell lung tumor), Neoplastic mammary ca, pancreas ca Hypothyroidism, diabetes, Endocrine hypoparathyroidism, pheochromocytoma (MEN II B) Drug-induced Anti-depressants, narcotics, anti- cholinergics, laxative abuse, smooth muscle relaxants, vincristine Chagas, viral (CMV, EBV, HSV) Infectious Nonfamilial hollow visceral Hirschsprung’s disease, chronic idiopathic Idiopathic myopathy intestinal pseudo-obstruction Familial visceral myopathies Familial visceral neuropathies, von Familial (AD or AR), MNGIE (AR) Recklinghausen’s disease
Patiënt with CIPS Full thickness biopsy � � Hollow visceral myopathy DNA investigation � � Hollow visceral myopathy → → no DNA investigation → → possible � MNGIE syndrome → → DNA investigation possible → → � Myoneurogastrointestinal encephalopathy syndrome � Autosomal recessive � pseudoobstruction, periferal neuropathy, ophtalmoparese 1 th year recurrent UTI’s / constipation � � Profylaxis AB / lactulose 6 th year � � rectumsuctionbiopsy (-) � Antroduodenal manometry (+)
Patient with CIPS � Out patient visits: ???? � Bloodpicks: ???? � Admissions: ???? − Diagnostics, operation, dehydration, application stoma’s, application broviac, application shunt…infection − 4x ic admission, infection � Radiology (79x): − X-thorax, X-Abd, MRI, CT-scan, US � Surgery 20x − Laparoscopy (full thickness biopsies), 2001 broviac catheter (TPN), application PEG and ileostoma, 2005 subtotal colectomy (distended colon, impaction with mucus), 2011 small bowel resection
Normal Gastrointestinal Motility Components Nerves Interstitial Cells of Cajal Muscles
Interstitial cells of Cajal and nerve cells controlling smooth muscle contractility neuron C O ACh NO Interstitial cell Smooth muscle cells
Mutation of the proto-oncogene c-kit blocks development of interstitial cells and electrical rhythmicity in murine intestine W/W V mutant +/+ wild type Ward et al., 1994
Anti c-kit-antibody (ACK2) treatment blocks development of ICC resulting in disturbed motility and distention of the gut Control ACK2 treated Torihashi et al., 1995
Congenital Motility Disturbances Causes Nerves Neuropathy Muscles Myopathy ICCs I CC “disorders”
Definition CIPS • Recurrent episodes of abdominal pain and distention of the abdomen resembling mechanical obstruction • No mechanical cause (endoscopy/radiology) • Distended bowel loops, with fluid levels • Absence of organic, systemic or metabolic diseases Stanghellini et al Clin Gastroenterol Hepatol 2005
Congenital Motility disturbances Clinical presentation • Presentation frequently in the neonatal period (80%) • Myopathy presents often already in utero − Bowelobstruction, megabladder
CIPS Symptoms • Recurrent/ continuous signs of obstruction • Symptoms age related / part GI tract − Abdominal distention 88% − Vomiting 72% − Constipation 61% − Abdominal pain 45% − Failure to thrive 31% − Diarrhea – bacterial overgrowth 28% − Dysphagia 3%
CIPS Clinic Symptoms from birth 50% Prenatal megacystis 30% Intestinal obstruction 100% Surgery 90% Urinary tract infections 90% Bacterial overgrowth 90%
CIPS Clinical presentation • Alarm symptoms − Recurrent/ continuous episodes of obstruction − Chronicity − Generalised gastro-intestinal dysmotility − Other organs affected • megacystis/ hydroureter / hydronefrosis) − Familiar − Recurrent non-diagnostic laparotomy
CIPS Diagnosis and investigation • Radiology X-Abdomen − Contrast X-Ray − • Surgery Avoid if possible − Full thickness biopsy −
CIPS Diagnosis and investigation • Test gastrointestinal motility Marker studies − Manometry (Oesofagus, − Antroduodenal, Colon) Electrogastrografy (EGG) − Scintigrafy − • Histopathology
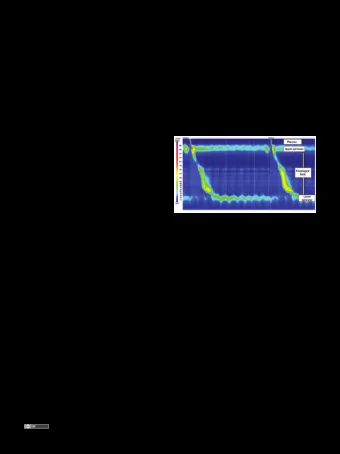
CIPS Diagnostics No sign of mechanical obstruction Small bowel manometry Myopathy Neuropathy Abnormal coördination, Normal coördination, normal amplitude contractions Low amplitude contractions
Normal antroduodenal motility Motility during fasting Postprandial
Small bowel manometry
Myopathy
CIPS Management
Multi-disciplinary treatment • Dietitian • Specialized nurses • Social worker • Psychologist • Home nurses • Pediatric surgeon • Neonatologist • Gastroenterologist
CIPS Management • Gastric tube • Nasoduodenal tube • Stimulation of motility (massage, medication) • Diet (low fiber and fat intake)
CIPS Nutrition • PEG gastrostomy • Jejunostomy • Home TPN 55% • Home TPN + enteral 35% • Enteral feeding 10%
CIPS Medication • Erytromycine − Stimulates gastric emptying − Stimulates antral contractions
CIPS 98 Laparotomies in 46 patients Reinterventions Intestinal adhesions 17 Redo enterostomy 12 Enterostomy prolapsus 7 Colectomy + ileo-rectal pull-trough 9 Pyloroplasty and gastrostomy 4 Nissen fundoplicatur 1 Goulet O et al 2001
Surgery in pseudo-obstruction G-J Tube SHORTENING THE GUT feeding venting Jejunal Tube Ileostomy
CIPS Prognosis • Overall moderate! • Mortality 10% – 30% − Iatrogenic complications • Sepsis / liver failure • Small bowel transplantation − 1/3 dies before transplantation • Prognosis − Poor – neonatal onset, urinary tract involvement, repeat surgery, myopathic disorders − Good – presence of normal peristalsis (manometry)
CIPS (prognosis) n = 105 • 18 months TPN 30% • Ileostomy/colostomy/jejunostomy 50% • Mortality (1mth - 7 yr) 15% Faure et al Dig Dis Sci 1999;953-9
CIPS (prognosis) n = 44 • TPN dependent 25% • Ileostomy/colostomy/jejunostomy 75% • Mortality 25% Heneyke et al Arch Dis Child 1999;81:21-7
CIPS : intestinal transplantation Decision criteria • Permanent intestinal failure • Permanent obstruction / aspiration • High level of PN dependency • End stage liver disease • Vascular complications • Very poor quality of life
CIPS : intestinal transplantation Overall results are poor and reasons are not fully analyzed
CIPOS : intestinal transplantation • Incidence of IF related complications including end stage liver cirrhosis • Multiple pre-Tx surgical procedure • Risks related to the Tx procedure
CIPOS : long-term outcome N = 85 Myopathy Neuropathy Indeterminate n=32 n=48 n=5 62.5% post Tx death No SBTX SBTX SBTX No SBTX SBTX n=29 n=3 n=3 n=45 n=2 Death Death Death Death Death n=7 n=3 n=1 n=10 n=1 Mousa H et al. Dig Dis Sci. 2002
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries