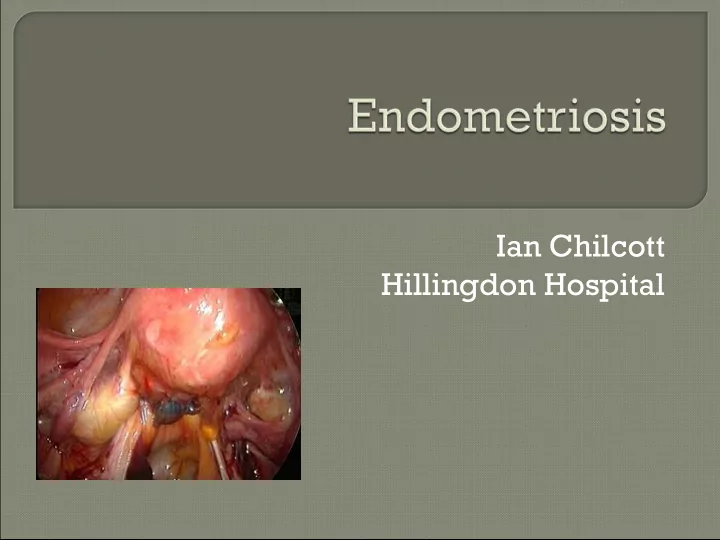
Ian Chilcott Hillingdon Hospital
Defined as the presence of endometrial- like tissue outside the uterus, which induces a chronic, inflammatory reaction Most common sites Ovaries Pouch of Douglas Uterosacral ligaments Pelvic peritoneum Prevalence 8-10% est
Aetiology Retrograde menstruation Coelomic metaplasia Genetic Altered immune function
Symptoms Dysmenorrhoea Deep dyspareunia Chronic non menstrual pain Dyschezia Cyclical rectal bleeding Infertility
Association with infertility Endometriomas/ severe anatomical distortion accepted Minimal/mild peritoneal disease less clear
Association with ovarian cancer Lancet Oncology Feb 2012 Meta analysis of 13 case control studies 13000 controls 8000 with ovarian cancer Relative Risk of clear cell carcinoma 3 low grade serous 2 endometrioid 2
Diagnosis Examination pelvic tenderness fixed retroversion tender USL visible lesions vagina cervix Exam may be normal
Diagnosis Investigations Ultrasound – endometriomas MRI CA-125 Laparoscopy – gold standard
Treatment Based on - symptoms - presence/absence of endometriomas - concern re fertility Empirical treatment without referral may be appropriate
Medical treatment Analgesia Hormonal treatment COCP Continuous until wish to conceive Cileste, Yasmin POP Cerazette Mirena If breakthrough bleeding, add cerazette or Cileste GnrH analogues +/- addback Danazol
Referral criteria Endometrioma on U/S Infertility Pt wanting definite diagnosis Failure of empirical treatment
Surgery Laparoscopic preferred At time of diagnostic lap Ablation/excision stage I-III – reduces pain at 6/12 compared to no treatment Fertility ablation & adhesiolysis I-II enhances fertility more than no treatment (Cochrane 2010)
Endometriomas Endometriomas
Hysterectomy /BSO Assisted reproduction IUI I-II IVF
Subfertility Endometriomas Patient prefers definite diagnosis Failure of empirical treatment Suitable empirical treatments NSAIDS COCP – continuously POP Mirena – add POP/COCP if not amenorrhoeic
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries