How to Establish a Multi ‐ ‐ How to Establish a Multi Hospital STEMI Transfer System Hospital STEMI Transfer System Dr. Greg Mishkel for the Doctors of Prairie Cardiovascular and in collaboration with our Community & Springfield Hospitals
MI: Evolution of care in Central Illinois •1990’s early adoption/promotion of iv thrombolyis = “drip & ship” •2000 adoption of mechanical reperfusion • 2002: Establish Institutional processes for acute MI care • 2005: DANAMI/PRAGUE/MHI model: Inter-hospital transfer to TWO Springfield hospitals (St. John’s Hospital, Memorial Medical Center) = PRAIRIE STAT HEART PROGRAM Barriers to PPCI STEMI Care in Central Illinois Barriers to PPCI STEMI Care in Central Illinois •Limited facilities •Limited facilities •Long inter-hospital travel distances •Long inter-hospital travel distances •Limited ACLS EMS accessibility •Limited ACLS EMS accessibility •Variability in ED services (locum tenens) •Variability in ED services (locum tenens)
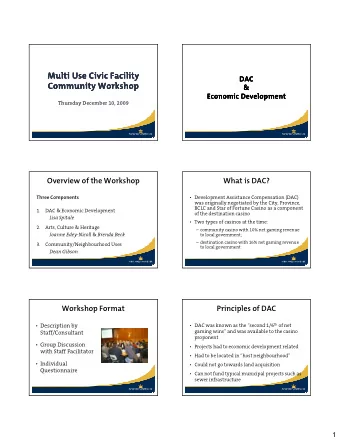
2005: 6 Referral Centers Mean Transfer Distance: 46 miles (range:28-88) 4: Helicopter, 2: Ambulance 2009 2009
So how was this done? Physician leadership, physician buy in Full time co ‐ ordinator/facilitator (communications, logistics, deal with “SNAFU’s”, educational events) Hospital commitment (funding, quality, cath lab personnel) Establish effective high quality ER STEMI program Establish lines of communication (ER switchboard cath lab) Treatment guidelines Monitor outcomes, modify procedures Reduce readmissions Build on success of local program to entice outside programs to be “part of the team” Regular (annual?) of all participants (we include the switchboard operators) in educational forums/updates to share results/successes/challenges
What do all of these first 3 requirements have in common PEOPLE NOT STRUCTURES Dofasco Steel my first summer job in Hamilton, Ontario “Our product is Steel…Our Strength is People”
So how was this done? Physician leadership, physician buy in Full time co ‐ ordinator/facilitator (communications, logistics, deal with “SNAFU’s”, educational events) Hospital commitment (funding, quality, cath lab personnel) Establish effective high quality ER STEMI program (St. John’s * 90) Establish lines of communication (ER switchboard cath lab) Treatment guidelines Monitor outcomes, modify procedures Reduce readmissions Build on success of local program to entice outside programs to be “part of the team” Regular (annual?) of all participants (we include the switchboard operators) in educational forums/updates to share results/successes/challenges
STEMI: Where We Started at our hospital Doing well: performing above the average hospital for STEMI care in Crusade and NRMI registries, but wanted to be exceptional Formation of AMI Team in 2003 to target performance above the top 10% of Crusade/Action registry hospitals Formal Intervention started late 2003/early 2004 Obstacles to performance improvement included distance of new ED from cath lab, lack of standardized protocols and medical record documentation.
AMI Team Strategic Goals Achieve D2B time of <90 minutes for 100% of STEMI patients Implement standardized, evidence based and guideline driven pathways of care to improve quality Achieve 100% compliance with admission and discharge medications for all AMI patients Achieve results above the top 10% of Action registry hospitals for STEMI care EKG done within 5 minutes for patients with chest pain ED Door to cath lab arrival of < 30 minutes Cath Lab arrival to balloon dilatation of < 25 minutes Implement pre ‐ hospital ECG
Methods Formation of a multidisciplinary AMI team with quarterly meetings in Fall of 2003 ED meds bundled ‐ ASA, Beta Blocker, Heparin, and Nitroglycerin ED physician empowered to concurrently activate cardiologist and cath lab team upon diagnosis of STEMI with STAR 90 page Cardiologist meets and evaluates patient in cath lab, not ED Accountability and tracking form following patient through process allowing evaluation of performance of various phases of the D2B process Implementation of guideline driven treatment protocol and procedural protocol Weekday night team resides in hospital Benchmarking of performance with other centers using Action and MIDAS registries.
AMI Team Dr. Charles Lucore, Chairman, Department of Cardiology Dr. Linda Nordeman, Chairman, Department of Emergency Medicine Dr. Greg Mishkel and Frank Mikell, PCCL Dr. John Nester, Springfield Clinic Dr. John Byrnes, Emergency Room Cardiac Catheterization Lab Representatives: Sheryl Friedrich et al Emergency Department Representatives: Amy Jones et al Cardiac Nursing Representatives: Jennifer Cullen et al Quality Resource Management Representatives: Diane Tebrugge et al Health Information Management Representatives: Heather Shankland et al
AMI Door to Cath Lab Tracking Sheet To be completed only for ST elevation and/or LBBB on 1 st 12 ‐ lead EKG patients Arrival Time __________ EKG Time ___________ Tech __________ Time Cardiologist paged __________ ED Physician ________ Time Cardiologist returns page _______ Cardiologist _________ Cath Lab notified __________ Cath lab responds _____ Pt prepared for cath lab _________ ED Nurse __________ Time Cath Lab calls for patient ________ Pt leaves ED ___________ Cath lab arrival time ________ Balloon inflation time ________ Complications that may delay process (pt requires intubation, pt arrests, or requires additional stabilization, atypical presentation) _________________________________________________________ _________________________________________________________
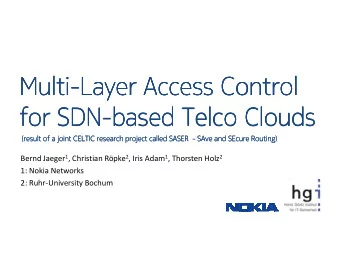
Acute Myocardial Infarction Discharge Medications 2003 – May 2009 (Data from NRMI 4, Action, MIDAS Comparative Performance System (CPMS)) 100 95 90 Aspirin 85 Beta Blocker Ace Inhibitor 80 Statin/lipid 75 ASA 99% Beta Blocker 98% 70 Ace/ARB 97% Statin 99% 65 2003 2004 2005 2006 2007 2008 2009 Top 10% (Action STEMI rpt) ASA 100% Beta Blocker 99% Ace/ARB 95% Statin 97% ACE #s do not always screen for LVEF < 40% from NRMI report
STEMI Myocardial Infarction In-Hospital Events (last 12 months) St. John’s National Avg. Top 10% Death Rate (%) 2.8% 5.9% 5.8% Door to Balloon Time (minutes) 54 71 59 Bleeding Requiring Transfusion (%) 2.3% 6.3% 7.4% Stroke 0.60% 0.80% 0.60% Length of Stay (days) 3.6 4.4 4.6 Source: 2 nd Qtr 08 - 1 st Qtr 2009 ACTION Registry ( Get With the Guidelines ) Gold Performance Achievement Award for 2009
So how was this done? Physician leadership, physician buy in Full time co ‐ ordinator (communications, logistics, deal with “SNAFU’s”, educational events) Hospital commitment (funding, quality, cath lab personnel) Establish effective high quality ER STEMI program Establish lines of communication (ER switchboard cath lab) Treatment guidelines Monitor outcomes, modify procedures Reduce readmissions Build on success of local program to entice outside programs to be “part of the team” Devise (based on local needs) an integrated/consistent one call, one protocol Regular (annual?) of all participants (we include the switchboard operators) in educational forums/updates to share results/successes/challenges
Global Components of Process of Transfer STEMI Care Tertiary Facility Community Facility Transport Door In-Door Out Departure-Door 2 Door 2-Balloon ECG Cath Lab Arrival Transfer Decision Diagnostic Cath Air Treatment PCI Ambulance Initiate STAT Heart Arrange Transfer Ideal <30 minutes <30 minutes <30 minutes Goal: Goal: Door-Balloon: ≤ 90 min .
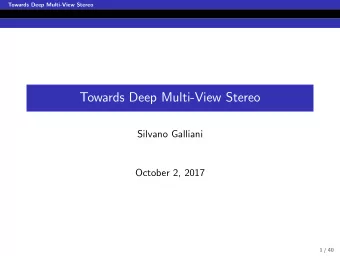
• Suspected MI (Step1 ) 3- 5 min • 12 Lead ECG/STEMI Identified (Step 2) • Determine Bleeding Risk (Step 3 ) Activate Call for quickest available Call Springfield Hospital 5-10 min Stat Heart transport ( Step 4) Activate Team Ambulance/Helicopter Stat Heart Team 15-20 min Low Bleeding Risk High Bleeding Risk Springfield Stat Heart Team Community 30 minute Transport 30 minute Transport Cardiologist Stat Heart time Available time NOT Available Coordinator Team Cath Lab Security ED MD PCI Protocol Contraindication Protocol Thrombolytic Protocol Admitting 2-RN Air/Ground Air/Ground Air/Ground Administrative Ancillary staff Transport Transport Transport Rep ER contact Goal: Out the Door in < 30 minutes
Lisa Page, RN Prairie Stat Heart Protocols
Goal out the door in 30 minutes or less 0-3 minutes Patient presents with chest pain or associated symptoms TREAT ALL patients as potential Stat Heart until deemed otherwise 3-5 minutes ECG done ECG to ED physician for quick diagnosis. ED physician determines if STAT Heart criteria is met. 5-12 minutes Activate STAT Heart team at community hospital (staff pre-assigned duties) First call -staff calls quickest transport air or ground (base on mileage between hospitals) Second call – Springfield Hospital receiving pt. Stat Heart team activated in Springfield. Automatic - accepting Prairie cardiologist and bed assigned.
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries