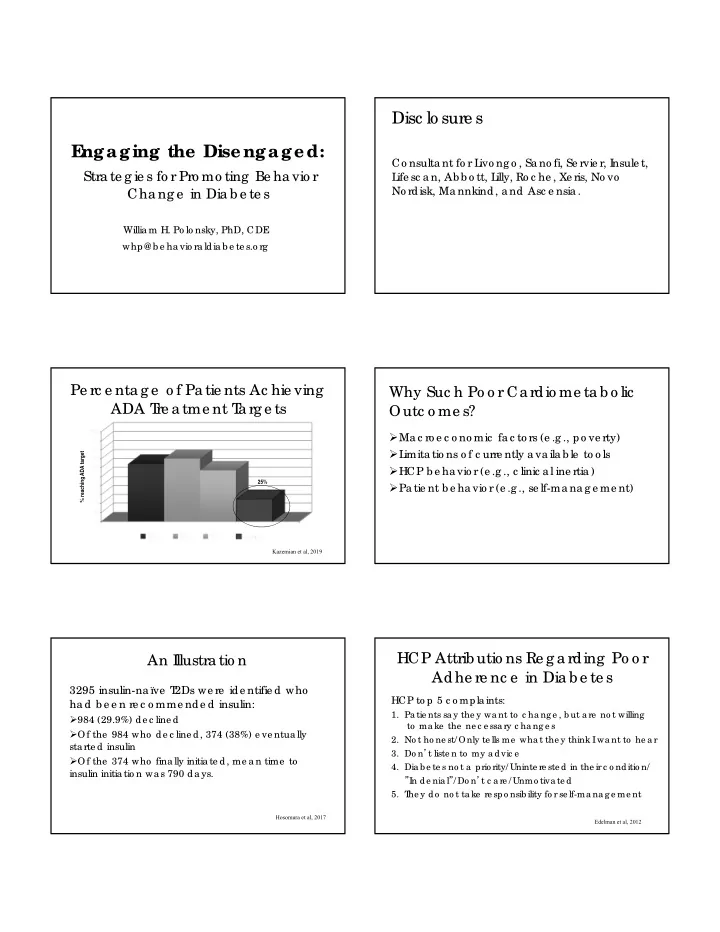
Disc lo sure s E ngaging the Disengaged: Co nsulta nt fo r L ivo ng o , Sa no fi, Se rvie r, I nsule t, Stra te g ie s fo r Pro mo ting Be ha vio r L ife sc a n, Ab b o tt, L illy, Ro c he , Xe ris, No vo No rdisk, Ma nnkind, a nd Asc e nsia . Cha ng e in Dia b e te s Willia m H. Po lo nsky, PhD, CDE whp@ b e ha vio ra ldia b e te s.o rg Pe rc e nta g e o f Pa tie nts Ac hie ving Why Suc h Po o r Ca rdio me ta b o lic ADA T re a tme nt T a rg e ts Outc o me s? Ma c ro e c o no mic fa c to rs (e .g ., po ve rty) L imita tio ns o f c urre ntly a va ila b le to o ls % reaching ADA target HCP b e ha vio r (e .g ., c linic a l ine rtia ) 25% Pa tie nt b e ha vio r (e .g ., se lf-ma na g e me nt) Kazemian et al, 2019 HCP Attrib utio ns Re g a rding Po o r An I llustra tio n Adhe re nc e in Dia b e te s 3295 insulin-na ïve T 2Ds we re ide ntifie d who HCP to p 5 c o mpla ints: ha d b e e n re c o mme nde d insulin: 1. Pa tie nts sa y the y wa nt to c ha ng e , b ut a re no t willing 984 (29.9%) de c line d to ma ke the ne c e ssa ry c ha ng e s Of the 984 who de c line d, 374 (38%) e ve ntua lly 2. No t ho ne st/ Only te lls me wha t the y think I wa nt to he a r sta rte d insulin 3. Do n ’ t liste n to my a dvic e Of the 374 who fina lly initia te d, me a n time to 4. Dia b e te s no t a prio rity/ Uninte re ste d in the ir c o nditio n/ insulin initia tio n wa s 790 da ys. ” In de nia l ” / Do n ’ t c a re / Unmo tiva te d 5. T he y do no t ta ke re spo nsib ility fo r se lf-ma na g e me nt Hosomura et al, 2017 Edelman et al, 2012
Re a l L ife with Dia b e te s 1. L iving with dia b e te s c a n b e to ug h It is a time -c o nsuming jo b Re a l L ife with Dia b e te s 1. L iving with dia b e te s c a n b e to ug h It is a time -c o nsuming jo b It is a b a la nc ing a c t tha t re q uire s vig ila nc e a nd a n a b ility to de a l with frustra tio n
Mo tiva tio n in Dia b e te s No o ne is unmo tiva te d to live a lo ng a nd he a lthy life T he re a l pro b le m: Ob sta c le s to se lf-c a re o utwe ig h po ssib le b e ne fits And the re a re a T ON o f o b sta c le s! T he unde rlying the me to mo st o b sta c le s is a la c k o f “wo rthwhile ne ss” L a c k o f Wo rthwhile ne ss L a c k o f Wo rthwhile ne ss An invisib le a nd no n-urg e nt dise a se An invisib le a nd no n-urg e nt dise a se Ho pe le ssne ss “Look, I’ll start worrying about my diabetes as soon as something “What’s the difference? This something falls off.” disease is going to get me no matter what I do. L a c k o f Wo rthwhile ne ss An invisib le a nd no n-urg e nt dise a se Ho pe le ssne ss Disc o ura g e me nt “I did everything I was supposed to, and now you’re telling me I have to take even more medications?!”
Wha t I s Dia b e te s Distre ss? Dia b e te s Distre ss T he fe lt b urde n o f living with a to ug h, Dia b e te s distre ss de ma nding dise a se T ype 1 dia b e te s (n = 224): 42% De spa ir: “I will e nd up with se rio us lo ng -te rm T ype 2 dia b e te s (n = 36,998): 36% c o mplic a tio ns, no ma tte r wha t I do ” L inke d to se lf-c a re a nd g lyc e mic c o ntro l Disc o ura g e d: “I a m o fte n fa iling with my Dia b e te s distre ss is o fte n c hro nic dia b e te s” Of tho se with e le va te d distre ss a t b a se line : 74% Ove rwhe lme d: “T his is ta king up to o muc h o f re ma in e le va te d le ve ls a t 9 mo nths. my me nta l a nd physic a l e ne rg y e ve ry da y” Polonsky et al, 1995; Polonsky et al, 2005 Fisher et al, 2016; Perrin et al, 2017 Pa tie nt-HCP Co mmunic a tio n So Wha t T o Do ? A vide o e xa mple ……… Dia b e te sdistre ss.o rg Ste p 1. Asse ss • T 1-DDS & DDS in E ng lish & T he info rma l a ppro a c h: Spa nish “Wha t’ s o ne thing a b o ut dia b e te s tha t’ s driving • Auto ma tic a lly sc o re d, with yo u c ra zy? ” printa b le T he fo rma l a ppro a c h: re po rts Use se lf-re po rt instrume nts
Dia b e te sdistre ss.o rg A T 1-RE DE E M Pa rtic ipa nt “ I t wa s to ta lly une xpe c te d a nd surprising . I ha ve ha d dia b e te s fo r 35 ye a rs. I n a ll tha t time no o ne ha s e ve r a ske d me wha t it wa s like fo r me to ha ve dia b e te s a nd wha t it wa s a b o ut dia b e te s tha t I fo und mo st distre ssing . And e ve n if the y did a sk, I do ub t tha t the y wo uld ha ve ta ke n the time o r ha d the inte re st to liste n c a re fully to my a nswe r.” HCP E mpa thy a nd He a lth Outc o me s Ste p 2. Re spo nd with E mpa thy Do n’ t try to fix yo ur pa tie nt’ s fe e ling s A re la tive ly re c e nt lite ra ture re vie w inc lude d 7 studie s (UK , US, a nd the Ne the rla nds): I nste a d, liste n, a c kno wle dg e a nd no rma lize “Give n the na ture o f dia b e te s, fe e ling this wa y is “T he re is a g o o d c o rre la tio n b e twe e n HCP e mpa thy pe rfe c tly re a so na b le a nd ma ny o the r pe o ple a nd pa tie nt sa tisfa c tio n a nd a po sitive re la tio nship fe e l the sa me .” with stre ng the ning pa tie nt e na b le me nt. E mpa thy lo we rs pa tie nts' a nxie ty a nd distre ss a nd de live rs sig nific a ntly b e tte r c linic a l o utc o me s” Derksen et al, 2013 Co nsulta tio n a nd Re la tio na l E mpa thy Ho w g o o d wa s yo ur HCP a t: 1. ma king yo u fe e l a t e a se 2. le tting yo u te ll yo ur sto ry 3. re a lly liste ning 4. b e ing inte re ste d in yo u a s a who le pe rso n 5. fully unde rsta nding yo ur c o nc e rns 6. sho wing c a re a nd c o mpa ssio n 7. b e ing po sitive 8. e xpla ining thing s c le a rly 9. he lping yo u to ta ke c o ntro l 10.ma king a pla n o f a c tio n with yo u Dambha ‐ Miller et al, 2019 Dambha ‐ Miller et al, 2019
HCP E mpa thy a nd Mo rta lity Outc o me s “I n this 10-ye a r fo llo w up o f pa tie nts with ne wly dia g no se d type 2 dia b e te s, tho se re po rting b e tte r e xpe rie nc e s o f e mpa thy in the first 12 mo nths a fte r dia g no sis ha d a sig nific a ntly lo we r risk (40% to 50%) o f a ll- c a use mo rta lity o ve r the sub se q ue nt 10 ye a rs c o mpa re d with tho se who e xpe rie nc e d lo w pra c titio ne r e mpa thy.” Dambha ‐ Miller et al, 2019 Ste p 3. Ma ke the I nvisib le Visib le Back on Track Feedback Name: Molly B. Your Targets Last Results FID #: Tests SAFE : At NOT SAFE : Your score or better Not yet at should be than goal goal A1C 7.0% or less 8.7% x Blood 130/80 125/75 x Pressure LDL 100 or less 116 x Ste p 3. Ma ke the I nvisib le Visib le Ste p 3. Ma ke the I nvisib le Visib le Be no n-judg me nta l. Be no n-judg me nta l. F Offe r c o ng ra tula tio ns whe n po ssib le . e a r ta c tic s ma y b e c o unte rpro duc tive : “Do yo u wa nt to g o b lind, do yo u? ” “Yo ur A1C is still to o hig h. “Its g re a t tha t yo u to o k the “I f yo u do n’ t do b e tte r, yo u’ ll e nd up o n insulin. Do n’ t yo u unde rsta nd time to g e t yo ur A1C do ne I s tha t wha t yo u wa nt, is it? !” VS. the c o nse q ue nc e s? to da y. T he numb e rs ha ve n’ t Ra the r tha n de sc rib ing numb e rs a s “g o o d/ b a d” Why a re n’ t yo u wo rking mo ve d muc h, whic h te lls us ha rde r o n this? ” tha t so me thing diffe re nt is o r “hig h/ lo w”, use “sa fe / unsa fe ”. ne e de d.”
F a c t Che c k Ste p 4. Sha re the Go o d Ne ws Q. Dia b e te s is the le a ding c a use o f a dult b lindne ss, a mputa tio n, a nd kidne y fa ilure . T rue o r fa lse ? T his do e sn’ t T his do e s me a n: me a n: g o o d c a re with g o o d c a re , A. F a lse . T o a la rg e e xte nt, it is po o rly c o ntro lle d will guar dia b e te s tha t is the le a ding c a use o f a dult antee odds ar e good b lindne ss, a mputa tio n a nd kidne y fa ilure . tha t yo u will no t yo u c a n live a de ve lo p lo ng , he a lthy life We ll-c o ntro lle d dia b e te s is the le a ding c o mplic a tio ns c a use o f… NOT HI NG! with dia b e te s 1D Co mplic a tio ns Afte r 30+ Ye a rs T 1D Co mplic a tio ns Afte r 30+ Ye a rs T % of patients with this complication % of patients with this complication Deckert et al, 1978 DCCT/EDIC Research Group, 2009 Hear t Attac ks in T ype 2 Diabetes What About T ype 2 Diabetes? Rate per 10,000-person years Rawshani et al, 2018
Hear t Attac ks in T ype 2 Diabetes Hear t Attac ks in T ype 2 Diabetes Rate per 10,000-person years Rate per 10,000-person years Rawshani et al, 2018 Rawshani et al, 2018 Move to Sweden! Hear t Attac ks in T ype 2 Diabetes Rate per 10,000-person years Rawshani et al, 2018 We E ve n Put it o n Mug s! Diabetes and Your Health “ To live a long and healthy life, develop a chronic disease and take care of it. ” ‐ Sir William Osler
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries