RBWH HD Clinic and Palliative Care Pathway Presented by: Lily Tang (Clinical Nurse) Date: 18/08/2016
RBWH HD Clinic History Flashback • First set up in 1994 by Psychiatrist Dr Lawrence and Neurologist Dr Lander- research focus (HSG data collection) with the help from HD Coordinator I. Simpson. • 2001- 2002 Dr J O’Sullivan, Dr R. Marsh and neuropsychologist -public clinic at Neuro Dept RBWH- increased clinical emphasis. • 2005 Speech pathologist C Barrett joined the clinic – funded by the Huntington’s Disease Association Queensland (now Huntingtons Queensland). • 2007 Welfare officers started attending the clinic • Genetic Health Queensland works separately – predictive/diagnostic testing+ genetic counseling
RBWH Clinic Now • MDT clinic consist of: -Neurologist, Registrar, +/- fellow -Psychiatrist, Registrar -Neuropsychologist, +/- student -Clinical nurse -Speech pathologist -Client service staff from HDQ -+/-Research fellow One stop shop for HD patients and their families.
What do we do in clinic? • Multidisciplinary holistic care approach • Provide clinical diagnosis • Drug therapy to reduce the burden of symptoms, maximize function and improve quality of life • Manage crisis, provide education, counseling and support for patients and carers • Advise on prognosis • Carry out various assessments of cognition, speech and swallowing • Refer to formal OT driving test if indicated • Discuss advance care planning, financial planning and family planning • Support and promote coordinated care with pt’s local health care providers, link pt in with support services • Offer access to research project that will improve the understanding and treatment for people with HD
Who do we see in clinics? • We see adult patients who have been genetically or clinically diagnosed with Huntington’s Disease, these include: - presymptomatic pts - early stage HD - mid stage HD - late stage HD • Pts with suspected HD without a clear family Hx should to be referred to GHQ, General Neurology clinic or Movement Disorder clinic to establish their diagnosis.
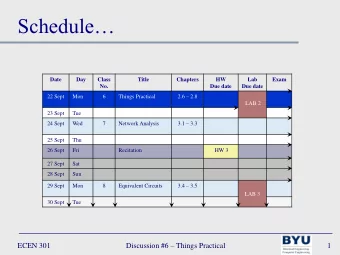
When and where are HD clinics held? • Monthly clinic (excluding public holidays) at Neurology Outpatient Department, RBWH • Contact details: Tel: (07) 3646 3111 Email: hdclinic@health.qld.gov.au
Referral Process • All new referrals need to be sent to Central Patient Intake (CPI) Unit via http://www.health.qld.gov.au/metronorth/refer/ Or via fax: 1300 364 952 Or by mail to: Metro North Central Patient Intake Unit Level 9 Block 8, Royal Brisbane & Women’s Hospital, Butterfield St, Herston QLD 4029 • Review pt’s referral needs to be updated 12 monthly by their GP.
Why HD needs a palliative approach? Huntington’s Disease Prolonged & Progressive Life threatening unpredictable disease neurodegenerative No cure complications disease trajectories Active treatment Palliative care approach +
Goals of Palliative Approach • To identify and respect a person’s wishes • To improve/maintain comfort and function • To address their psychological, spiritual and social needs • To support them on their journey through curative care, palliative goals and preparation for death • To provide support for their family and carers [Ref 1,4,17]
How do we find out a person’s wishes? -Advanced Care Planning (ACP) • EPOA 1 • AHD 2 • Statement of choices 3 Please contact Office of Advance Care Planning:(07) 3646 5000 https://mycaremychoices.com.au [Ref 12]
Nursing interventions for some challenging symptoms of end stage HD Pain Emotional, Psychosocial, Communication Spiritual care Chorea End stage HD & Rigidity+ Badykinesia Agitation ADLs Restlessness Aggression Falls
[Ref 7,8,9,18 ] Pain
Communication tips • Only ask one question at a time • Keep it simple, ask Yes/No questions Eg. Are you in pain? • Avoid open ended question, allow choices, but limit options Eg. What do you want to wear today? Do you want to wear pants or shorts? • Reduce environmental distractions (turn TV/radio off) • Allow time for response- do not rush the speaker, always explain what you are doing • Have a routine- let pt know what is expected, stick to the routine • Encourage pt to speak clearly and slowly, one word at a time, say/spell the main word • Utilise body gestures or communication aids for nonverbal pt • Ask pt look or point to what they want • Refer to a speech pathologist for further assessments and strategies [Ref 2,3,5,6,10,16]
ADLs tips • Hygiene care V.S • Involve pt and family in decision making, work to share common expectations, establish tailor made, flexible, innovative and consensus-based nursing care plan
Falls and injury prevention Safety acceptable risks • Environmental modifications a. reduce clutter in the room b. stabilise furniture so it won’t move c. anti-slip mat, d. make sure floor is not wet e. night light in the toilet f. adjust bed height g. alarming system, “sensor mat, or invisa - beam” h. protective equipment: padded guardrail, helmet, hip protector, HD bed etc. i. avoid restraints [Ref 3,4,5,10]
Agitation, Restlessness and Aggression Management • Set routines and rules • Listen to their concerns and demands • Speak in a low soft voice • Keep environment calm • Look for triggers/escalators, avoid them, observe visual cues, know when to stop • Acknowledge pt’s anger/ frustration, redirect them from source of anger • Allow time for response • Contact DBMAS + SBRT 1800 699 799, 24/7 helpline for over the phone advice & in home assessment [Ref 2,3,5,6,10]
Emotional, Psychosocial and Spiritual care • Emotional, psychosocial and spiritual care: - Complex family dynamics -Fractured families, multiple affected members, repeated losses -Guilt, regret and sadness -Reduced family support -Underlying psychiatric and cognitive impairments complicates their emotional responses and how we support them - Be sensitive and honest, being there, stay with the pt, carry out pt’s wishes • Supporting family and carers Video: https://youtu.be/RedG8rt_SQY [Ref 2,3,4, 5,6,10]
End of Life Care Options • What are the options for HD patients when they suffered from a life threatening complication and reached terminal stage of their life? At home- with palliative care support RACF Hospice Hospital
End-of-life Care at Home • What services are available when you want to care for someone dying at home? - GP - Community-based palliative care services, http://palliativecare.org.au/im-a-health-professional/# - Community outreach services - Domestic assistance – including personal care, cleaning, washing and cooking etc. Carer’s support and respite care - - PalAssist Palliative Care Helpline 24/7- 1800 772 273 [Ref 4,5,6,10]
End-of-Life Care in RACF • The Residential Aged Care End of Life Care Pathway (RAC EoLCP) was developed by the Brisbane South Palliative Care Collaborative (BSPCC). • The RAC EoLCP is an evidence based care plan designed to guide the provision of good quality end of life care in residential aged care. • It improves the outcomes for dying residents and enhances the quality of the care provided by residential aged care staff. • The pathway can be accessed via https://metrosouth.health.qld.gov.au/raceolcp [Ref 1,7,11,14,15]
The entire document forms part of the resident’s medical record. • The RAC EoLCP is a 12-page document, divided into 5 sections to facilitate comprehensive planning delivery evaluation and documentation of end of life care provided to dying residents. • The entire document forms part of the resident’s medical record. [Ref 11]
When to commence RAC EoLCP? • According to ‘Guidelines for a Palliative Approach in Residential Aged Care’, it is appropriate to start the pathway if three or more of these signs and symptoms are applicable to the resident (Australian Government Department of Health and Ageing, 2006). 1. Experiencing rapid day to day deterioration that is not reversible 2. Requiring more frequent interventions 3. Becoming semi-conscious, with lapses into unconsciousness 4. Increasing loss of ability to swallow 5. Refusing or unable to take food, fluids or oral medications 6. Irreversible weight loss 7. An acute event has occurred, requiring revision of treatment goals 8. Profound weakness 9. Changes in breathing patterns [Ref 14]
End of Life Care in Hospital • The Clinical Guidance for the Dying Patient (CgDp) is developed by RBWH Palliative Care Service and the Clinical Pathways team, Health Service and Clinical Innovation Division. • It has been approved for statewide use within Queensland Health hospital facilities. • It guides healthcare professionals to focus on care in the last hours or days of life. • It enables the delivery of high quality care tailored to the patient’s individual needs, when death is expected. [Ref 13]
CgDp
Conclusion The dying process is unique to each person but in most cases, a plan of care can be put in place to support the patient, doctors and nurses, relatives/friends to achieve the best quality of care at the end of life.
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries