Preventing Paediatric Window Falls: A Collaborative Approach to Effecting National Building Code Change December 3, 2019 12:00 PM EST Dr. Michelle Simonelli and Mr. Bruce Schultz T HIS WEBINAR IS BEING RECORDED . S TAY IN THE L OOP ! T HE SLIDE DECK AND RECORDING WILL BE WWW . FALLSLOOP . COM EMAILED AFTER THE WEBINAR . WWW . JR . FALLSLOOP . COM
Preventing Paediatric Window Falls: A Collaborative Approach to Effecting National Building Code Change December 3, 2019 12:00 PM EST Dr. Michelle Simonelli and Mr. Bruce Schultz T HIS WEBINAR IS BEING RECORDED . S TAY IN THE L OOP ! T HE SLIDE DECK AND RECORDING WILL BE WWW . FALLSLOOP . COM EMAILED AFTER THE WEBINAR . WWW . JR . FALLSLOOP . COM
Preventing Paediatric Window Falls A COLLABORATIVE APPROACH TO EFFECTING NATIONAL BUILDING CODE CHANGE DR. MICHELLE SIMONELLI, MD, FRCPC MR. BRUCE SCHULTZ, CODES OFFICER
Objectives ▪ Identifying The Problem → City of Calgary ▪ Collecting The Data: → Numbers → Injury Patterns ▪ Journey To Change The National Building Code ▪ Next Steps ▪ Building Partnerships Outside The Health Care/IP community
Identifying The Problem
Identifying The Problem ▪ The Building Code is less restrictive for single and two family houses than for multifamily houses ▪ Wind ndow w sills for for ope penabl ble wi windo dows ws can n be be at at fl floo oor r level vel
Identifying The Problem ▪ Building Code not treating similar hazards the same
Proposed Change to National Building Code Existing Code with Proposed Change: Effectively: 5) Windows need not be protected in accordance with Sentence (4), ▪ Openable able wind ndow in a singl gle e or two r two where the bottom edge of the openable portion of the window is a) more than 900 mm above the finished floor, or the window serves family ly re residenc dence e to be the same e as fo for r a dwelling unit that is not located above another suite , multi-famil family dwell llin ings gs re requiri ring: ng: a) the window serves a house with a secondary suite , b) the only opening greater than 100 mm by 380 mm is a horizontal opening at the top of the window, • Guard c) the window sill is located more than 450 mm above the finished • Limiter (permanent) rmanent) floor on one side of the window, or d) the window is located in a room or space with the finished floor • Minimum 900mm (35”) openable sill described in Clause (d) b) located less than 1 800 mm above the floor or ground on the other side of the window. above floor OR OR (See Note A-9.8.8.1.(4).) • Maximum 1800mm (70”) openable sill above grade
But Where’s the Data?: The Beginning of an Intra-Professional Alliance ▪ City of Calgary approached ACH Trauma Director ▪ Required data to demonstrate severity of problem ▪ Required assistance from the medical community to advocate for urgent change
Pedi diatric tric Inj njur ury y in n Cana nada: da: Le Leadi ding ng Cause se of of Death
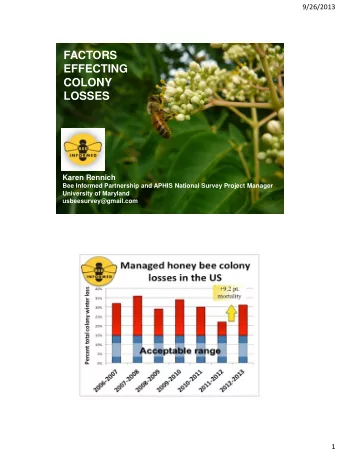
Canadian Pediatric Falls ▪ As with adults, falls are the leading cause of injury admissions & ED visits in Canadian children ▪ 42% of injury related hospitalizations ▪ 36% of injury related ED visits
Pediatric Window Falls In 2016, 23% of ACH Major Trauma Patients were injured in a fall ➢ 56% of these falls were multi-storey falls from windows ▪ Why does it happen? How big is the problem nationally? ▪
Problem Scope: National Data Sources I. Canadian Institute for Health Information (CIHI) ➢ National Ambulatory Care Reporting System (NACRS) ➢ The Hospital Morbidity Database (HMD) ➢ The Discharge Abstract Database (DAD) II. Canadian Hospital Injury Reporting and Prevention Program (CHIRPP via PHAC)
CHIRPP ▪ 19 national CHIRPP ED sites ▪ Front of form collects descriptive data by pt ➢ Date, location, sport/MVC (protective equipment), free text description of injury ➢ Rich descriptive qualitative data ▪ Back of form injury data by HCP ➢ Nature of injury, body part, disposition, follow up ▪ Entered into eCHIRPP database ▪ Site or nationwide queries
CIHI National Data: Pediatric Falls from Buildings ▪ Annually, 124 children ages 0-9 admitted for falls from buildings ▪ PQ: 31* ▪ BC:31 ▪ ON:27 ▪ AB: 14 ▪ SK: 5 ▪ MB: 5 ▪ NS: 3 ▪ NB:3 ▪ NWT, NFLD, Nunavut: 1 each
National Pediatric Window Falls Ages 0-9 Years Year ADMIT ITTED D AFTER EST. ADMITTED D EST. . ED VIS ISIT ITS S FALL FROM M AFTER FALL AFTER FALL FROM ▪ 70% of falls from BUIL ILDING FROM M WIN INDOW WIN INDOW buildings were falls 2011 483 from windows 138 97 2012 420 120 84 ▪ 20% of children 2013 392 112 78 seen in ED were 2014 434 124 87 admitted 2015 450 128 90 2016 420 120 84 TOTAL 742 520 520 2599 2599 AVERA RAGE GE 124 87 87 433 33
Limitations of the Data ▪ Robustness of NACRS and DAD ▪ Provincial annual counts less than 5 are suppressed ▪ “Jurisdictions that choose to participate” ▪ NACRS & DAD data indicate Ontario has less 2 x the number of window falls of Alberta despite having 3.3 times the population
Limitations of the Data
Windows and Balconies Falls related Pediatric Injuries in Northern Alberta, Kundra M. and Craig, W. Retrospective review & 2 year prospective study at Stollery 2009-2017 ▪ 107 falls (15.2 per year) <17 yrs ▪ Mean age 5.14, Median age 4, Mean height 110.8cm ▪ 63.2% boys ▪ 55.7% fell in own home ▪ 50.5% through window screen ▪ Only 20% had sills higher than ‘knee height’ ▪ 28.6% had furniture pushed up to the window ▪ 28.3% were admitted
Demographics of Pediatric Window Falls ACH ▪ 66% are 4 years of age or less ▪ 78% are 5 years of age or less ▪ Majority are boys ▪ Majority fall from their own homes
Admission Rates and Injury Patterns ▪ 28% admitted to Alberta Children’s Hospital or Stollery ▪ Skul kull l fra ractu tures es & tra rauma matic tic bra rain in inj njur uries es (TBI)* BI)* Cervical spine fractures ▪ ▪ Facial and long bone fractures Splenic or liver lacerations ▪ ▪ 53% of Stollery admissions required surgery ▪ 72% treated & discharged from ED ▪ 13% ACH ED discharges required specialist follow up
Costs of Pediatric Window Falls Human Cost Health Care Costs ▪ Direct and Indirect Costs ▪ In 2010, falls for children 0-9 years cost $1,000,000,000 ▪ Multi storey falls are the most severe pediatric falls ▪ Most children admitted after multi storey falls are <5 an and have a TBI The younger er the patien ent, t, the higher er the costs
The Journey to Change the National Building Code: ▪ Why change the National Building Code? ▪ The National Building Code is the model code for Canada ▪ Each province chooses how to adopt the code in their jurisdiction
The Journey to Change the National Building Code:
The Journey to Change the National Building Code Formulate Proposal 09/2012-09/2015 Gather support from medical Submit Code Change Request community 11/2016 Provincial (CCR) to NRC process in NRC forwards to Standing 12/2016 parallel Committee (SC) SC forwards to Task Group 04/2017 (TG) TG Recommends to SC 05/2018 To public review 10/2018 TG reviews public review 04/2019 comments 05/2019 TG Recommends to SC SC recommends to CCBFC approves inclusion 06/2019 Commission (CCBFC) in code
The Journey to Change the Building Code ▪ What needs to be addressed in a code change request ▪ What is the problem? ▪ What is the proposed solution and how does it address the problem ▪ Which of the stated objectives and functional statements of the code will the proposed solution assist in achieving? ▪ What are the cost benefit implications ▪ What are the enforcement implications
The Journey to Change the NBC Responses Supportive of change as proposed 103 Supportive of change with minor 9 potential modifications Non supportive/ request 2 modifications
Slow road to change ▪ 14,072,080 Canadian dwellings ▪ 8,000,000 (60%) single or duplex dwellings ▪ In 2018: 80,000 single & duplex housing starts ▪ New Code for new construction → ▪ 1% of current single & duplex housing inventory ▪ Not all provinces will adopt NBC immediately ▪ Not all the current housing stock has non conforming windows ▪ New Code also applies to renovations ▪ Architectural changes with new National Energy Standards (smaller windows)
Next Steps: Existing Dwellings ▪ After market devices available that meet recognized standards
Next Steps: Existing Dwellings ▪ Install guards or limiters restricting opening to 4” (10 cm) ▪ Close & lock windows with low sill heights when small children in house ▪ Don’t push furniture up against windows ▪ Understand that screens are NOT safety devices
Next Steps: Existing Dwellings
Next steps: Public Awareness
Next Steps: Public Awareness
Next Steps: More Codes to Be Changed.. ▪ It’s long. It’s complicated. It’s unwieldy. YEARS. ▪ It takes an expert with the seat at the table, like Bruce.
Building Partnerships: The NRC Framework
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries