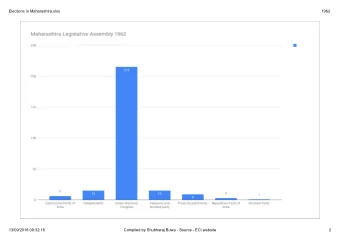
A descriptive study and evaluation of a contemporary team based model of care introduced by Australian emergency departments in response to time based access targets By Jane Senior ECI Advanced Trainee
Introduction • Who am I? • Why research team based care?
Methods • Literature research ‐ only 4 papers identified as relevant, none of which were Australian based • Pilot Study ‐ 3 known ED
Objectives • To describe a new “team based” model • To describe any changes to routinely collected ED performance data • Discover other information including perceived effectiveness and impact on ED quality of care
Study design • Retrospective descriptive study • Survey ‐ 24 questions • ED directors or representative • 35 ED invited to participate ‐ included Top 10 major metropolitan and major regional of the National Health Performance Authority ranking of ED by compliance with NEAT Jan ‐ March 2013 ‐ other ED known • 20 confirmed to be working in a TMOC and agreed to participate in study
Emergency Departments Surveyed • The majority of the surveys were completed by the director of ED (13/18) • 5 of the 7 states/territories were represented Most were mixed departments • (12/18), the remainder seeing adults only • Majority of ED working in TMOC are classed as major referral (12/18) Majority saw >60,000 patients • per annum (14/18)
Reasons for changing to TMOC • 10/18 had only been working in a TMOC in the last 12months 5/18 in 1 ‐ 3 years • 3/18 greater than 3 years • “ many issues were seen as driving this- clearly NEAT”, “ expectations from admin about meeting NEAT” and “ Essentially imposed from above”.
The Team Half the teams were made up of Doctors only and the other half composed of Doctors and Nurses.
Who participates in the team • Average number of total members in the team for doctors was 5 in both the day and evening shifts and 3.7 during the night shift. (sample size 18) • The average number of nurses working in the team was 3. This was consistent at all times of day (sample size 9)
Operational information Patients were allocated Team members were identified geographically (8/18) or electronically (10/18), by coloured sequentially (8/18) stickers (7/18) and on the whiteboard (3/18) “ for the fast track patients are allocated “we use coloured labels that clasp onto the geographically but for the main uniform as the stickers stuck to the floor of the department they are allocated department instead!”. sequentially ”
During weekdays Monday • through Friday half (9/18) the ED worked 24 hours a day as a team with the other half (9/18) working extended hours (8 ‐ 23hrs) “variable and depended on available staffing” “not at all at weekends or on public holidays” • During the day there were many more teams with 5/18 having 2 teams, 8/18 having 3 teams, 4/18 having 4 teams and 1/18 had 5 teams.
Impact on ED performance data 16 14 12 10 8 Yes 6 No Don’t 4 know 2 0 NEAT overall increased Average time to being seen by a Doctor reduced %DNW reduced Time to admission decision from triage reduced Triage wait times reduced Doctors satisfaction improved Nurses satisfaction improved Doctors sick leave reduced Nurses sick leave reduced ED performance data
What is the most important aspect of making the TMOC work? “TBC needs both an adequate number of senior decision makers, and enough junior doctors to effect the instructions given” “adequate numbers of staff- junior and senior” “All the above are important- important not too fragment effort and concentrate in main ED where all can be monitored”, “all of the above are important parts of the model” “Executive buy-in”
When does the model become ineffective? Staffing Only 6 of the 18 employed more staff • less effective at night due to reduced numbers when there are members missing • “had employed more staff but that was to deal with increasing reduced junior staffing numbers make it • presentations not purely working in less effective the TMOC” • when not enough staff to put teams together “Currently requesting additional Night time ‐ less staff, more junior staff • registrar and nursing staff to make If the team is too small for the number of • model work better” patients it needs to see • Staff sick leave. Doctors then need to “this is the main reason why it has cover multiple areas had little impact” • Model suffers if one or more shifts unfilled due to roster shortages or sick leave • Yes, when there are doctors off sick
Senior role ED overloaded / surges • When the senior person on duty does not • at times of surge multiple patient moves support the role made double handling an issue • does depend on quality of registrar leadership • Periods of continuous peak demand in team ‐ we try to have a more experienced reg. • When surges of patients lead us to be on each team but leadership skills vary swamped • Don't always have ED consultant for every team where ED is overloaded and too many • • Sometimes when there are too many seniors in patients in the waiting room and no where to a team there is lack of clarity as to who the see them team leader actually is • doesn't work well when access blocked • There is an expectation that the juniors will do • We have 2 acute teams and one Fast Track / the "grunt work" after senior decision making Paediatric team, with slight staffing input differences....depending on the flux of • The seniors need to accept that 1: there should patients and which area is busy mismatch of be one defined leader for each period and this resources can be an issue. leader needs to be identified. 2: that they may • lack of flow have to assume primary care for patients • sudden influx of patients, the teams become overwhelmed. This is a common occurrence. Bizarrely, sometimes less pressure on individual teams to function. Individual team • members may not realise that department out of control
What can be done to improve the model? Staffing Team adequate staffing • • more direct supervision of the team approach increased senior staffing, • • team specific stats more senior staff, • consistent senior staff • greater seniority of the team leaders • Beds improve sick leave cover • • ED renovation/redesign could improve • bigger teams to help with surges geographical team based care • 24/7 flow coordinators better inpatient buy in • • more nurses enough beds in ED • • extend to nursing staff (but they are fixed available inpatient beds • on geographical allocation rather than team) • We are about to trial a geographical model in the main arena with a team of doctors/nurses per side
89% believed that the TMOC had improved the quality of care in the ED I think it makes it much more personal Team care as opposed to sequential care • • experience for junior medical staff and they means that the patient is not endlessly tend to identify with their team ‐ I think a repeating the same story. well functioning team provides better • There is some healthy "competition" to quality care ensure that your team's patients are seen • 15% improvement in NEAT overnight from and sorted and there is some anecdotal 55% to 70% Sustained and improved evidence that this improves overall (range 70 ‐ 80%) since. Average LOS compliance. decreased 1 hour!! (saving of 200 pt hours Team based models work as long as there • per day) is work done around leadership and role • But not all of the Emergency Physicians delineation. believe this to be the case • Teams in Emergency departments are • much better accountability, less hiding often dynamic in view of the individual from workload, early decision making and members. involvement of seniors, better work flows It is important that the team leaders • • Clear communication and tasking are understand the needs of the team and are important. effective in coordinating activity in order to be efficient as well as effective • It is much easier to manage a small group of 4 ‐ 5 clinicians rather than 15 ‐ 18.
Conclusions • 89% felt working in a TMOC had improved quality of care in ED • Larger ED • Average size of the team 5 ‐ 9 participants although not enough information to make recommendations about size or makeup • Adequate staffing and an effective Senior leader are seen to be a strong marker to make the model work
Acknowledgements • NSLHD Human Research Ethics Committee • Dr. Sally McCarthy – ECI • Matthew Murray – ECI • Dr. Robert Day – RNSH • Dr. Paul Preisz – St Vincent’s • Dr. de Villiers Smit – The Alfred
Questions?
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries