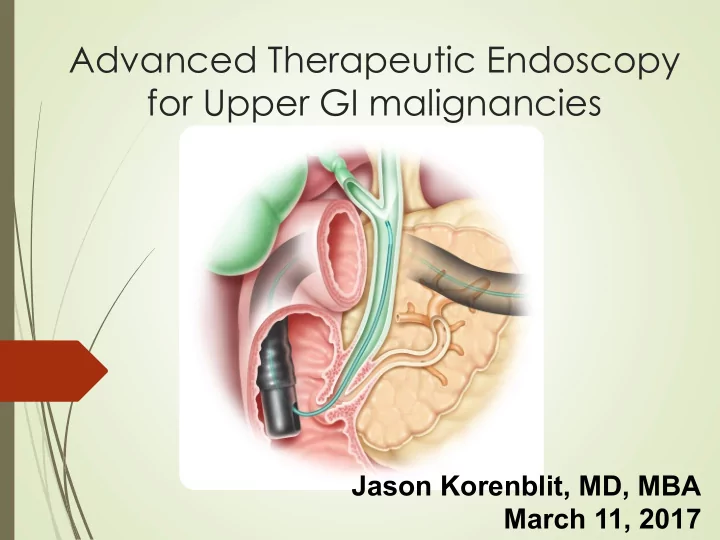
Advanced Therapeutic Endoscopy for Upper GI malignancies Jason Korenblit, MD, MBA March 11, 2017
Disclosures ´ Financial disclosures: None, unfortunately. 2
Educational Objectives ´ Available Devices and Modalities ´ Staging EUS ´ Therapeutic EUS ´ Endoscopic mucosal resection ´ ERCP and Cholangioscopy ´ Deep enteroscopy
Endoscopic Ultrasound Radial scope – Curvilinear scope – Probe-based – diagnostic only diagnostic and diagnostic only therapeutic
EUS and staging
Esophageal Cancer Staging ´ EUS is the most accurate modality for locoregional T staging ´ 80-90% ´ In one metaanalysis, AUROC 0.96 ´ T1(a) lesions can be endoscopically resected ´ Nodal staging ´ Endoscopic criteria ´ width greater than 10 mm ´ round shape ´ smooth border ´ echo-poor pattern ´ 80-100% predictor of nodal mets when all four present.
Restaging After Neoadjuvant Therapy Restaging after resection: Sen 92% Spec 96%
Thoracic EUS ´ Mediastinum ´ Lymphoma ´ Thymus cancer ´ Metastatic Disease ´ Lung tumors ´ Posterior and inferior mediastinum ´ EBUS better for superior and anterior ´ Hilar lesions near the esophagus ´ Sampling of pleural effusions ´ Node Sampling ´ Celiac staging
EUS in the Stomach ´ T1 vs T2 ´ Sen 85%, Spec 90% ´ T1 tumor limited to submucosa or shallower amenable to endoscopic resection ´ T1/2 vs T3/4 tumor ´ Sen 86, Spec 90% ´ EUS imaging alone can detect nodes as well as CT but DOES NOT predict malignancy well ´ Specificity only 67%, heterogeneous studies ´ EUS/FNA of nodes preferred ´ Stromal lesions benefit from EUS to determine what layers they arise in ´ EUS/FNA for tissue
Hypoechoic lesion arising in Needle in mass the muscularis propia
Endoscopic Mucosal Resection ´ Esophagus ´ Barrett’s nodule ´ T1A adenocarcinoma ´ Less than 2cm ´ Less than 1/3 circumference of the lumen ´ Stomach ´ Stromal tumors and adenocarcinoma limited to submucosa ´ 3% recurrence in Japanese literature ´ Large lesions may benefit from Endoscopic submucosal dissection for en bloc resection ´ Duodenum ´ Much higher perforation rate ´ Colon ´ Very amenable but watch for signs of muscularis propia invasion ´ Failure to lift ´ Depression
Traditional Saline/Fluid Lift
Cap-assisted Saline Lift
Band-assisted EMR
Defect Closure Clips Endoscopic Suturing
Pancreatic EUS ´ Staging data is very mixed in pancreas ´ T staging accuracy 63-67% ´ N staging accuracy 44-66% ´ Assessing vascular invasion ´ Data actually shows EUS getting WORSE over time ´ Likely due to quality of the studies ´ Much better for portal vein and splenic art/vein than SMA/SMV ´ EUS is better than CT for detection of small lesions (98% vs 86%), about the same for nodes (about 47%), about the same for determining resectability (accuracy around 90%)
Who needs an FNA? ´ Tissue prior to Chemo/XRT ´ Advanced disease/Nodes ´ Poor surgical candidate ´ Metastatic disease ´ Resectable patient with small tumor (and no jaundice?) ´ Traditionally right to surgery ´ FNA can be helpful ´ Neuroendocrine tumors ´ Lymphoma ´ Autoimmune pancreatitis ´ Chronic pancreatitis ´ Sens 92%, Spec 96% ´ Accuracy 91% in patients without risk for chronic pancreatitis
Normal HPB Anatomy
Traditional ERCP vs Cholangioscopy ´ Fluoroscopy only ´ Fluoroscopic guidance/blind sampling ´ Wire manipulation using 2D image only ´ Needs Contrast ´ Video Cholangioscopy adds ´ Direct biopsy/sampling ´ Direction of wire under combined visual and fluoroscopic guidance ´ Can limit contrast injection and possibly prevent infection ´ Ability to discern malignancy vs benign disease using imaging ´ Precise guidance of certain therapies
Pancreaticobiliary Cancers ´ Liver tumors ´ Primary HCC ´ Metastatic tumors ´ Cholangiocarcinomas ´ Hilar tumors ´ Extrahepatic ´ Intrahepatic ´ Pancreatic ´ Gallbladder ´ Ampullary
ERCP with Brush Cytology AUTHOR / PATIENTS SENSITIVITY SPECIFICITY YEAR N (%) (%) Ponchon, 1995 233 35% 97% Lee, 1995 149 37% 100% Ornellas, 2006 50 40% 100% Jailwala, 1999 133 30% 100% TOTAL 565 36% 99% Fukuda – Gastrointestinal Endoscopy Volume 62, No. 3, 2005 “The most convenient and widely used method for tissue sampling from the biliary stricture and a filling defect is brushing cytology . However, the sensitivity and the negative prediction values are insufficient for deciding the treatment plan.”
ERCP with Fluoroscopically Guided Biopsy AUTHOR / PATIENTS SENSITIVITY SPECIFICITY YEAR N (%) (%) Ponchon, 1995 128 43% 97% Schoefl, 1997 103 65% 100% Jailwala, 2000 133 37% 100% TOTAL 364 48% 99% Ponchon - Gastrointestinal Endoscopy December; 42(6):565-72 “Conclusions: Endobiliary sampling is technically difficult and has a limited sensitivity for the diagnosis of malignant biliary stenosis.”
Intraductal Papillary Mucinous Tumor ´ Mucinous tumor formed in the cells lining pancreatic duct ´ Typically causes pancreatic duct to dilate which obstructs flow of pancreatic juices to duodenum ´ Precursor to cancer IPMT
Catheter-Based Cholangioscopy ´ Single operator ´ Similar size to mother/daughter scope ´ Video imaging ´ 1.2mm accessory channel ´ Disposable ´ 4 way tip deflection
Clinical Application of Technology ´ Stones ´ Choledocholithiasis ´ Intraductal stones ´ MPD stones
Clinical Application of Technology ´ Strictures ´ Benign ´ Malignant
Clinical Application of Technology IPMN Biliary Anastomosis
Efficacy ´ ERCP with brushing alone or with fluoroscopic biopsy ´ Sensitivity 30%-50%, specificity 95%-99% ´ ERCP with Cholangioscopy alone ´ Meta-analysis of 8 prospective studies ´ Sensitivity 90%, specificity 87% ´ ERCP with cholangioscopy- directed biopsy ´ Sensitivity 69%, specificity 98% ´ Pancreatic strictures ´ IPMN’s detected in 95% of cases, benign strictures in 80%, cancers in 63% ´ Best for IPMN
Intraductal cholangiocarcinoma
Potential Complications of Cholangioscopy ´ Pancreatitis ´ Perforation ´ Hemorrhage ´ Hematoma ´ Septicemia/infection ´ Cholangitis ´ Allergic reaction to contrast medium
Small Bowel Evaluation ´ Video Capsule ´ Non-invasive ´ 60% detection rate in all lesions/bleeding sources ´ No therapy possible ´ Push Enteroscopy ´ Up to 80cm past the Ligament of Trietz ´ Colonoscope or dedicated enteroscope ´ Potentially therapeutic
Deep Enteroscopy Balloon-Assisted Enteroscopy Spiral Overtube Enteroscopy
Deep Enteroscopy ´ Requires general anesthesia (usually) ´ Time consuming – 60 to 120 minutes ´ Up to 360cm past Ligament of Treitz antegrade ´ Up to 180cm from the ileocecal valve retrograde ´ 30% failure rate! ´ Possible to see the entire GI tract with both exams ´ 70-86% in Japan, 4-63% in US/Europe ´ Due to combination of experience and patient size
Summary and Recommendations ´ When in doubt, refer for EUS ´ Nodules ´ Extrinsic GI lesions ´ If it is within 7cm of the upper GI tract, we can hit it ´ Combination of EUS and EMR is effective for the management of early mucosal lesions and obviates surgery ´ Therapeutic ERCP can be used to establish diagnosis and palliate the patient ´ Deep enteroscopy can be used to obtain tissue reliably to the mid-small bowel
References Osanai M, Itoi T, Igarashi Y, et al. Peroral video cholangioscopy to evaluate indeterminate ´ bile duct lesions and preoperative mucosal cancerous extension: a prospective multicenter study. Endoscopy 2013; 45:635. Lee YN, Moon JH, Choi HJ, et al. Direct peroral cholangioscopy using an ultraslim upper ´ endoscope for management of residual stones after mechanical lithotripsy for retained common bile duct stones. Endoscopy 2012; 44:819. Sasahira N, Isayama H, Nagano R, et al. Noncalcified pancreatic stone treated with ´ electrohydraulic lithotripsy using SpyGlass pancreatoscopy. Endoscopy 2011; 43 Suppl 2 UCTN:E272. Shah RJ, Chen YK. Transpapillary and percutaneous choledochoscopy in the evaluation ´ and management of biliary strictures and stones. Techniques in Gastrointest Endosc 2007; 9:161. Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy system ´ for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointest Endosc 2007; 65:832. Brauer BC, Chen YK, Shah RJ. Single-step direct cholangioscopy by freehand intubation ´ using standard endoscopes for diagnosis and therapy of biliary diseases. Am J Gastroenterol 2012; 107:1030.
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries