
Adult Growth Hormone Deficiency: How to Incorporate Guidelines into - PDF document
1/25/20 UCSF CME Pituitary Disorders: Advances in Diagnosis and Management San Francisco, CA Saturday January 25, 2020 Adult Growth Hormone Deficiency: How to Incorporate Guidelines into Clinical Practice Kevin C.J. Yuen, MD, FRCP(UK), FACE
1/25/20 UCSF CME Pituitary Disorders: Advances in Diagnosis and Management San Francisco, CA Saturday January 25, 2020 Adult Growth Hormone Deficiency: How to Incorporate Guidelines into Clinical Practice Kevin C.J. Yuen, MD, FRCP(UK), FACE Professor of Medicine and Medical Director Barrow Neurological Institute Pituitary Center St. Joseph’s Hospital and Medical Center University of Arizona College of Medicine and Creighton School of Medicine Phoenix, AZ 1 Disclosures • Received research grants to Barrow Neurological Institute from Ionis, Crinetics, Millendo, Corcept and Novartis • Served on Advisory Boards for Pfizer, Novo Nordisk, Ipsen, and Corcept 2 1
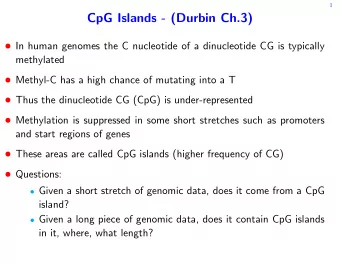
1/25/20 What are Clinical Practice Guidelines (CPG)? “Systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances.” (Institute of Medicine, 1990) • Most of the content are derived from extensive literature reviews • Reflects the state of the field at time of publication, and because changes in this area are expected, periodic updates may be implemented • Some recommendations may not be appropriate in certain situations Bottomline: use CPG in conjunction with best clinical judgment 3 GRS Workshop in Australia April 14-17, 1997 4 2
1/25/20 2007 Consensus Guidelines for the Diagnosis and Treatment of adults with GHD: GRS, ESPE, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society and Endocrine Society of Australia 5 2009 Medical Guidelines for Clinical Practice for GH Use in GH-Deficient Adults and Transition Patients: AACE 6 3
1/25/20 2011 Evaluation and Treatment of Adult GH Deficiency Clinical Practice Guideline: Endocrine Society 7 2016 Hormone Replacement in Hypopituitarism in Adults Clinical Practice Guideline: Endocrine Society 8 4
1/25/20 2019 Guidelines for Management of GH Deficiency in Adults and Patients Transitioning from Pediatric to Adult Care: AACE 9 Why another CPG in 2019? Summarize current knowledge of GH stimulation tests • • Summarize the increasing evidence of beneficial effects and long-term safety of GH replacement • Address skepticism about GH use: - high cost of therapy and its true benefits - difficulty conducting GH stimulation tests in the office - concerns about safety of long-term therapy - still a misconception of true adult GHD vs physiological decline in GH • Highlight several sub-populations of patients described to be “at risk” for adult GHD - how to test? - when and how to treat? Review the literature of GH use for conception and pregnancy • • Dispel the myth of using GH for sports and aging New developments • 10 5
1/25/20 Outline summary of the new AACE 2019 CPG 58 numbered recommendations: • - 12 Grade A (21%), 19 Grade B (33%), 21 Grade C (36%), and 6 Grade D (10%) • 13 question-based sub-sections • 357 references: - 51 (14%) EL 1 ( strong ) - 168 (47%) EL 2 ( intermediate ) - 61 (17%) EL 3 ( weak ) - 77 (22%) EL 4 ( no clinical evidence ) 11 Case 1: 57 y/o male with NFPA • TSS 3 years ago and SRS 2 years ago • Now has TSH and ACTH deficiencies (on stable doses of Levothyroxine and Hydrocortisone) • IGF-I SDS -1.5 • Healthy, except for possible childhood febrile seizures • Presents with a 10 lb (4.5 kg) weight gain over 6 months, and persistent fatigue • Family history of osteoporosis, hyperlipidemia and cancer Read on the internet and would like to be considered for GH 12 6
1/25/20 Case 1 discussion points • Why treat adult GHD? • Who to test for adult GHD? • Use of appropriate GH stimulation tests and cut-points • Interactions between GH and concurrent GCs and thyroid hormone • Safety concerns associated with long-term GH replacement • Use of GH for anti-aging 13 Why treat adult GHD? Body composition lean body mass • ¯ fat mass • Bone total body bone mass • BMD • Effects require >18–24 months treatment • Aerobic exercise capacity VO2 max (most studies) • Quality of life (QoL) in some aspects of QoL (proportional to degree of baseline impairment) • Improved surrogate CV risk markers ?Decreased mortality risk BMD, bone mineral density; QoL, quality of life. Simpson H et al. Growth Horm IGF Res 2002;12:1–33. 14 7
1/25/20 Potential impact of untreated GHD vs benefits of GH replacement on CV risk UNTREATED ADULT GHD REPLACEMENT CV RISK FACTORS CONVENTIONAL SURROGATE CV RISK MARKERS ¯ Lipids (total cholesterol, LDL, TG) ¯ CRP Pro-inflammatory cytokines (IL-6, TNF- a ) ¯ Glucose intolerance/hyperglycemia « β-cell function ¯ Adipokines (adiponectin , leptin / « ) ¯ Insulin resistance ¯ Pregnancy-associated plasma protein A ¯ Metabolic syndrome Coagulation system (pro-coagulation ) ¯ ¯ Endothelial dysfunction ¯ INCREASED INDIVIDUAL CV RISK IMPROVED CRP, C-reactive protein; CV, cardiovascular; GH, growth hormone; GHD, growth hormone disorder; LDL, low-density lipoprotein; TG, triglyceride; TNF, tumor necrosis factor. 15 Life expectancy in adults with NFPA receiving GH replacement therapy CI, confidence interval; GH, growth hormone; GHRT, growth hormone replacement therapy; NFPA, non-functioning pituitary adenoma Olsson DS et al. Eur J Endocrinol 2017;176:67–75. 16 8
1/25/20 17 Who to test for adult GHD? Acquired Congenital Skull-based lesions Genetic Pituitary adenoma, craniopharyngioma, Rathke’s cleft cyst, Transcription factor defects (PIT-1, PROP-1, LHX3/4, HESX-1, meningioma, glioma/astrocytoma, hamartoma, chordoma, PITX-2) lymphoma, metastases GHRH receptor gene defects GH gene defects Brain injury GH receptor/post-receptor defects TBI, sports-related head trauma, blast injury, perinatal insults Associated with brain structural defects Infiltrative/granulomatous disease Single central incisor Langerhans cell histiocytosis, autoimmune hypophysitis, Cleft lip/palate sarcoidosis, TB, amyloidosis Surgery to sella, suprasellar and parasellar region Cranial irradiation CNS infections Bacterial, viral, fungal, parasital Infarction/hemorrhage Apoplexy, Sheehan’s syndrome, SAH, stroke, snake bite Empty sella Hydrocephalus Idiopathic Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232. 18 9
1/25/20 Pulsatile pattern of 24-hr GH secretion in a 30 y/o vs 60 y/o healthy adult vs an adult with GHD 25 Sleep 30 yo healthy adult 20 60 yo healthy adult 15 GH ( µ g/L) Adult with GHD Random points of overlap with GH levels in healthy adults 10 05 0 09:00 21:00 09:00 Clock time GH, growth hormone; GHD, growth hormone disorder. 19 Serum IGF-I levels throughout life 640 Men (n = 81) 320 Women (n = 71) 160 IGF-I ( µ g/L) Normal range 80 40 IGF-I more reliable for screening for diagnosis 20 in young adults 10 10 20 30 40 50 60 70 80 90 100 Age (years) IGF, insulin-like growth factor. Hilding A et al . J Clin Endocrinol Metab 1999; 84:2013–9 20 10
1/25/20 AACE 2019 CPG algorithm for testing adult patients with clinical suspicion of GHD Adult patient with clinical suspicion of GHD Organic GHD Organic GHD History of hypothalamic-pituitary tumors, surgery, cranial ≥3 hormone deficiencies 0, 1 or 2 hormone deficiencies irradiation, empty sella, pituitary apoplexy, traumatic brain Low IGF-I (<−2.0 SDS) Low IGF-I (<0 SDS) injury, subarachnoid hemorrhage, autoimmune hypophysitis or Rathke’s cleft cyst No further testing Low suspicion Further testing High suspicion Normal IGF-I (≥0 SDS) required required Low IGF-I (<0 SDS) Treat Observe Further testing required Legend for GST Treat if: - peak GH ≤ 3.0 µ g/L in normal-weight (BMI < 25 kg/m 2 ) patients - peak GH ≤ 3.0 µ g/L in overweight (BMI 25-30 kg/m 2 ) patients ITT Macimorelin with a high pre-test probability GST Peak GH ≤ 5.0 µ g/L Peak GH ≤2.8 µ g/L - peak GH ≤ 1.0 µ g/L in overweight (BMI 25-30 kg/m 2 ) patients Yuen KCJ, et al. Endocr Pract. (see Legend) with a low pre-test probability Treat Treat 2019;25(11):1191-1232. - peak GH ≤ 1.0 µ g/L in obese (BMI > 30 kg/m 2 ) patients 21 Lower GH cut-point recommended for the GST ROC curve analysis to determine the GH cut-point for the GST Sensitivity Specificity GH, growth hormone; GST, glucagon stimulation test; ROC, receiver operating characteristics. Gomez JM et al. Clin Endocrinol (Oxf) 2002;56:329–34. 22 11
1/25/20 Previous GST studies suggesting the effects of central adiposity and glucose intolerance in decreasing peak GH levels Yuen et al. Pituitary 2013 Jun;16:220–30 Dichtel et al. J Clin Endocrinol Metab 2014 Dec;19:4712–9 Retrospective Diri et al. Pituitary 2015 Dec;18:884–92 Wilson et al. Growth Horm IGF Res 2016 Feb;26:24–31 Hamrahian et al. Pituitary 2016 Jun;19:332–41 Prospective GH, growth hormone; GST, glucagon stimulation test. 23 Mechanism of action of macimorelin Macimorelin acetate – + GHRH SRIF Hypothalamus + + Ghrelin Pituitary – gland GH – Stomach Liver IGF GH, growth hormone; GHRH, growth hormone-releasing hormone; IGF, insulin-like growth factor. Camina JP et al. Endocrine 2003 Oct;22(1):5-12. 24 12
Recommend




More recommend
Explore More Topics
Stay informed with curated content and fresh updates.