Sun and Statins What do vitamin D and statins have in common? Tristan Melton Pharmacy Resident 2011-12
Objectives 1) Gain an appreciation and understanding for the pathophysiology behind statin induced myopathies 2) Review the evidence behind vitamin D supplementation for prevention and resolution of statin induced myopathies
Statins By The #s All time best selling family of drugs • 20 billion dollars annually (2009) Most prescribed drugs in Canada • 12 million prescriptions in 2009 “ASA of the 21 st century”
Case: NM • 85 y/o ♂ ht: 178 cm wt: 90 kg BMI = 28.4 Admitted March 19 • Chief complaint: Shortness of breath • History of present illness: recently discharged for upper GI bleed with progressive shortness of breath and weakness over previous 4-5 days.
Case: NM PMH: • Upper GI bleed NSAID use – VGH March 7-15 • Coronary artery disease – Previous MI (1989) • Atrial fibrillation • Complete heart block pacemaker – Hx infected pacemaker (reimplantation 2007) • Aortic stenosis with aortic/mitral regurgitation • Background CHF with preserved systolic fxn
Case: NM PMH: • Hypertension • Dyslipidemia • Asthma (mild) • Hx of ARF secondary to gentamicin • Prostate cancer (radiation/hormone therapy) Surgery: hernia repair x 3, left total knee replacement, prostatectomy and multiple pacemaker procedures
Case: NM Social History: • Lives with wife in senior’s condo • Two daughters and one son • Retired truck driver and crane operator • Few glasses of wine/week • Previous smoker ≈ 13 years (quit >50 years ago) Allergies/Intolerances: • Penicillin? – rash 50 years ago • ACE inhibitors - dry cough
Case: NM Medications prior to admission (BPMH) • ASA 81 mg po daily • Telmisartan 20mg po daily as directed • Hydrochlorothiazide 25 mg po daily as directed • KCl 8meq po daily • Furosemide 40mg po daily • Rosuvastatin 40mg po daily • Ezetimibe 10mg po q2d • Pantoprazole 40mg po bid
Case: NM Medications prior to admission (BPMH) • Ferrous fumarate 300mg po bid • Advair inhaler – 500 mcg bid • Salbutamol inhaler – 200mcg q4h prn • Impatropium inhaler – 80mcg qid • Omega 3 supplement – 1 capsule po daily Vaccines up to date • influenza • pneumococcal
Case: NM Systems: Vitals: HR=76 BP=130/80 RR: 20 Afebrile Gross: pale, unwell, overweight CNS: decreased sleep quality of late Resp: increasing SOB, scattered crackles in lung bases MSK: marked fatigue unable to stand up – “stiff muscles” unable to bend arm – “crampy” hands and legs – limited left shoulder ROM
Case: NM LABS: Marker (range) 19 20 22 23 26 29 CK Total 3,973 2,897 1,029 371 (40-230 U/L) Myoglobin 8,603 1,677 (28-72 ug/L) Serum Creatinine 155 148 172 171 120 86 (60-100 umol/L)
Drug Therapy Problem a) NM is at an increased risk for significant morbidity/mortaltiy secondary to experiencing myositis/rhabdomyolysis which is most likely attributable to his statin therapy and would benefit from discontinuation of his rosuvastatin. b) NM is at a high risk to experience a cardiovascular event given his complex past medical history and would benefit from an assessment of his dyslipidemia management.
Other DRPs Anemia requiring Vitamin B 12 and iron supplementation Inappropriate use of Advair inhaler Reassessment of ipratropium Requires warfarin teaching Requires adequate calcium supplementation Adherence concerns from recent medication changes Increased risk for ARF secondary to ARB Increased risk to experience a fall secondary to BP
Goals of Therapy Health Care Team • Identify and resolve cause of myositis/rhabdomyolysis Decrease associated morbidity and mortality • Provide evidenced based medication to reduce future risk of cardiovascular events • Reduce/minimize any ADR with therapy • Adherence assessment Patient “I think your barking up the wrong tree” • Resolve current muscle stiffness/cramping • Increase strength • Minimize/eliminate adverse drug reactions • Have pharmacist prepare all meds for discharge!
Statin Induced Myopathy • Most common reason for discontinuation – Range very mild to severe signs/symptoms • Incidence around 5-15% • Two studies report repot a 1.5x increased risk of muscle complaints compared to those on placebo • Lower incidence in studies – Exclude high risk patients (previous myopathy) – Exclude those with potential drug interactions THIN database: fluvastatin>pravastatin>atrovastatin=rosuvastatin
Statin Induced Myopathy NM CK SrCr 3,973 172 Myositis ± ?rhabdo
Statin MOA a) HMG-CoA reductase inhibitors b) Atherosclerotic plaque stability
Statin Myopathy Mechanisms 1) Isoprenoid deficiency -by-products of HMG-CoA reductase pathway -deficiency disrupts cell apoptosis regulation & skeletal muscle cell structure
Statin Myopathy Mechanisms 2) CoQ10 inhibition -required for oxidative phosphorylatoin and ATP production -statins reduce CoQ10 by blocking mevalonate production
Statin Myopathy Mechanisms 3) Reduced sarcolemmal cholesterol -reduced cholesterol levels lead to alterations in myocyte membrane -Can cause modification in membrane integrity and fluidity destabilization
Statin Myopathy Mechanisms 4) Altered calcium homeostasis -secondary to increased expression of ryanodine receptors 3 (RR3) which are responsible for causing a marked increase in intracelluar calcium 5) Autoimmune -statin induced immune-mediated necrotizing myopathy -single nucleotide polymorphism (rs4363657 SLC01B1 gene on chromosome 12)
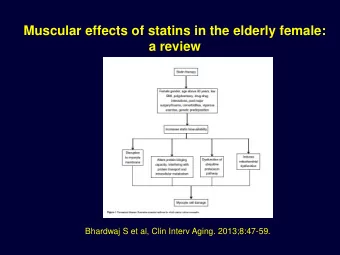
Statin Myopathy Risk Factors 1) Demographic – female, elderly, low BMI, frail, heavy exercise 2) Genetics -organic anion transporting polypeptides (OATP1B1) -cytochrome P450 system -glucuronidation -CoQ10 -inherited muscle diseases 3) Co-morbidities – excessive alcohol consumption, major surgery, previous/family hx myopathy, AKD/CKD, hypothyroidism QUIZ: Which two statins are minimally excreted in the urine?
Statin Myopathy Risk Factors 4) Pharmacokinetics 5) Dose Silva et al. through a meta-analysis showed an increased risk of high dose statin causes CK>10xUNL (OR 9.97 95% (1.28-77.92) p =0.028 6) Drug interactions
So Why NM? Demographic elderly ✓ Genetics unknown Co-morbidities alcohol hx ✓ Pharmacokinetics possibly Dose high ✓ Interactions ?pantoprazole, ?ezetimibe Research: Vitamin D insufficiency?
So Why NM? Academic request for vitamin D level Granted by geriatrician Marker (range) March 28 Vitamin D 25 (OH) 78 (75-150 nmol/L)
PICO Patient : experiencing myositis/rhabdomyolysis secondary to a statin Intervention : vitamin D supplementation Comparator : no therapy Outcome : Primary : resolution of vitamin D deficiency prevent statin-induced myalgia Secondary : adequate vitamin D levels reduce statin-induced myalgia
Vitamin D and Myopathy • First manifestation of deficiency myalgias • Serum levels are related to physical performance in elderly MOA: (hypothetical) • Interaction with statin on vitamin D deficient skeletal muscle fibers • “preferential shunting” for hydroxylation of vitamin D through CYP3A4 reducing availability for statin metabolism
Literature Search Search Terms : • Statin • Vitamin D • Myositis • Myalgia Databases : PubMed, Cochrane, Embase, Medline, IPA, Limits : none
Literature Search Results : • 5 prospective cohorts • 2 retrospective cohorts • 2 case reports
CMRO 2011: 1683-90
Glueck 2011 P : 150 /2,360 hypercholesterolemic pts (May 2007 – Jan 2011) • Inclusion – Serum vitamin D <32 ng/ml (80 nmol/L) – Previously taken or current use of statin – Myositis-myalgia causing cessation of statin therapy • Exclusion – Corticosteroids – Supplemental vitamin D at study entry – Co-morbidities muscle or bone pain » Diabetic sensory neuropathy, fibromyalgia, polymalgia rheumatica, arthritis, peripheral vascular disease, sensory neuropathy, hypothrodisim – Patients who refused vitamin D supplementation – Previously reported statin intolerant patients treated with Vitamin D
Glueck 2011 I : Rx for Vitamin D 50,000 IU 2/week x3weeks once weekly Statin restarted after 3 weeks C : prospective cohort O : Would vitamin D supplementation with resolution of vitamin D deficiency result in statin tolerance T : initial reassessment at 3 months, then q4 months
Glueck 2011 Results: Vitamin D (nmol/L) Duration VD Normalized Myositis- (months) Entry Follow-up (>80 nmol/L) myalgia free 11.5 52.4 104.8* 78% 87% ¶ * p <0.001 comparing study entry vs follow-up by paired Wilcoxon test ¶ Total cohort
Glueck 2011 Limitations: • Size • Non randomized, doubled blinded, placebo controlled trial • Patient population (young, generally healthy) • Duration of myositis-myalgia free • Single centre • Statin dose adjustments to reduce LDL • Myalgia vs. non-myalgic groups based on subjective reports • Definition of myositis-myalgia causing cessation of statin • Initial myalgia to higher doses of statins • 65% used rosuvastatin for statin reinstitution • Other lipid lowering medications in some patients • Increase in serum vitamin D secondary to statin (L, C)
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries