Role of ezetimibe in targeting residual risk Faculty Disclosure - PowerPoint PPT Presentation
Beyond statins: Role of ezetimibe in targeting residual risk Faculty Disclosure Declaration of financial interests For the last 3 years and the subsequent 12 months: I I have received a research grant(s)/ in kind support A From current
Beyond statins: Role of ezetimibe in targeting residual risk
Faculty Disclosure Declaration of financial interests For the last 3 years and the subsequent 12 months: I I have received a research grant(s)/ in kind support A From current sponsor(s) (MSD, Sanofi) YES B From any institution (Roche) YES II I have been a speaker or participant in accredited CME/CPD A From current sponsor(s) (MSD, Sanofi) YES B From any institution (Amgen) YES III I have been a consultant/strategic advisor etc A For current sponsor(s) (MSD, Sanofi) YES B For any institution (Pfizer, Amgen) YES IV I am a holder of patent/shares/stock ownerships A Related to presentation NO B Not related to presentation NO
Targeting residual risk Plaque rupture Cholesterol lowering Statin Plus Rx Statin Rx ACS Clinical event horizon Asymptomatic phase Modifiable residual risk Fatty streak Total modifiable Unstable risk lesion Non-modifiable residual risk Stable age, sex, genetics lesion 30 60 40 50 70 80 Age (years) After Packard CJ, Weintraub WS, Laufs U. Vascul Pharmacol. (2015); 71:37-9
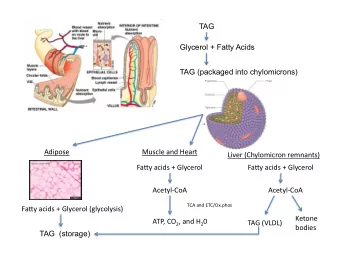
Impact of dual inhibition of cholesterol synthesis and absorption Dietary sources LDL x (1000 mg) 50% 500 mg Chol Ezetimibe 25% Chol x Chylomicron remnants Synthesis (1000 mg) (900 mg) Statin 1500 mg 500 mg
LDL-C and Lipid Changes 1 Yr Mean LDL-C TC TG HDL hsCRP Simva 69.9 145.1 137.1 48.1 3.8 EZ/Simva 53.2 125.8 120.4 48.7 3.3 Δ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5 Median Time avg 69.5 vs. 53.7 mg/dL Cannon et al. N Engl J Med. (2015) 372:2387-97
Individual Cardiovascular Endpoints and CVD/MI/Stroke HR Simva* EZ/Simva* p-value All-cause death 0.99 15.3 15.4 0.782 CVD 1.00 6.8 6.9 0.997 CHD 0.96 5.8 5.7 0.499 MI 0.87 14.8 13.1 0.002 Stroke 0.86 4.8 4.2 0.052 Ischemic stroke 0.79 4.1 3.4 0.008 Cor revasc ≥ 30d 0.95 23.4 21.8 0.107 UA 1.06 1.9 2.1 0.618 CVD/MI/stroke 0.90 22.2 20.4 0.003 *7-year 0.6 1.0 1.4 event rates (%) Ezetimibe/Simva Simva Cannon et al. N Engl J Med. (2015) 372:2387-97 Better Better
Mendelian randomisation 2x2 ‘trial’ of LDL lowering Meta-analysis of 14 studies, 108,376 subjects, 10,464 CHD events HMGR synthesis HMGR gene variants Referent (wild type) LDLc 0.09mmol/l lower variants CHD events 7.0% decrease 3-OH 3MG CoA mevalonate NPC1L1 Both NPC1L1 and NPC1L1 gene variants absorption HMGR variants LDLc 0.08mmol/l lower LDLc 0.17mmol/l lower CHD events 6.5% decrease CHD events 13.7% decrease Ference et al. Circulation. 2014;130; A19754
Lessons from clinical trials IMPROVE-IT total events analysis Murphy et al. J Am Coll Cardiol (2016);67:353-61
Long-term benefits of LDL lowering WOSCOPS 20-year followup CHD mortality All-cause mortality 12 45 Over entire period Over entire period Percentage with event 40 27% risk reduction 13% risk reduction Percentage with event 10 P<0.001 P<0.001 35 Placebo Placebo 8 30 25 6 Pravastatin 20 Pravastatin 4 15 Original trial 10 2 5 0 0 0 2 4 6 8 10 12 14 16 18 20 22 0 2 4 6 8 10 12 14 16 18 20 22 Years since randomisation Years since randomisation 55 65 75 y Average age of cohort Ford I et al. Circulation. (2016); 133:1073-80
WOSCOPS at 20 years In trial and post trial event rates In trial Post trial Placebo, Pravastatin, Placebo, Pravastatin, number (%) number (%) Adjusted Hazard number (%) with number (%) with Adjusted Hazard with event with event Ratio (95% CI) event event Ratio (95% CI) In trial event rates Total n = 3023 Total n = 3118 P-value* Endpoint Total n = 3293 Total n = 3302 P-value* 427 ( 14.13%) 372 ( 11.93%) 0.82 ( 0.71, 0.94) , Fatal or nonfatal MI 190 ( 5.77%) 115 ( 3.48%) 0.59 ( 0.47, 0.74) , (1989-1995) 0.0054 <0.0001 CHD related death 198 ( 6.01%) 119 ( 3.60%) 0.58 ( 0.47, 0.73) , 480 ( 15.88%) 418 ( 13.41%) 0.82 ( 0.72, 0.93) , or nonfatal MI <0.0001 0.0028 823 ( 27.92%) 739 ( 24.12%) 0.79 ( 0.70, 0.89) , CHD related death 273 ( 8.29%) 177 ( 5.36%) 0.58 ( 0.47, 0.72) , 0.0002 or hospitalisation <0.0001 1301 ( 46.05%) 1215 ( 41.51%) 0.81 ( 0.73, 0.90) , CV related death or 415 ( 12.60%) 329 ( 9.96%) 0.62 ( 0.52, 0.73) , <0.0001 hospitalisation <0.0001 Fatal or nonfatal 40 ( 1.21%) 29 ( 0.88%) 0.56 ( 0.31, 1.03) , 332 ( 10.61%) 329 ( 10.36%) 1.00 ( 0.82, 1.22) , stroke 0.0608 0.9856 Ford I et al. Circulation. (2016); 133:1073-80
Lessons from completed LDL lowering trials Risk reduction is related to LDL decrease Data from trials of:- • Statin vs placebo • More vs less intense statin therapy. Relative risk reduction • Combination therapy with ezetimibe Regression line reveals:- 1.0 mmol/l fall in LDLc translates into a 22% decrease in risk LDLc reduction (mmol/l) CTTC Lancet (2005) 367;1267-78 Cannon et al. N Engl J Med. (2015) 372:2387-97
Understanding the broader impact of LDL lowering in IMPROVE-IT CTTC regression 1 mmol/l drop in LDLc = 22% risk reduction Absolute CV risk 16 Real-world usage % with CV event 12 IMPROVE-IT 8 4 40 80 120 160 mg/dl R x -20% -20% 1.3 1.7 3.3 4.1 mmol/l CTTC Lancet ( CTTC Lancet (2010) 376;1670-81 LDL cholesterol Laufs et al EHJ (2014) Laufs et al EHJ (2014) Europ Heart J 35;1996-2000
NICE - Lipid lowering with ezetimibe Technology Appraisal Guidance - February 2016 • Ezetimibe monotherapy is recommended as an option for treating primary hypercholesterolaemia in adults in whom initial statin therapy is contraindicated or who cannot tolerate statin therapy. • Ezetimibe, co-administered with initial statin therapy, is recommended as an option in adults who have started statin therapy when: o LDL cholesterol concentration is not appropriately controlled either after appropriate dose titration of initial statin therapy or because dose titration is limited by intolerance to the initial statin therapy and o a change from initial statin therapy to an alternative statin is being considered NICE - Lipid modification in ACS – CG181: 2015 • Aim for >40% reduction in non-HDLc
Need for treatment options But cardiologist Dr Aseem Malhotra said: 'I have no doubt millions of people taking statins in the UK will not benefit but are being put at risk of unnecessary harm.' Concerns about statins were raised earlier this year by the Queen's former doctor, Sir Richard Thompson. May 15 th 2016
Options in optimal LDL/ nonHDLc lowering Patient not at goal for LDLc/ non-HDLc Further LDL reduction indicated clinically Combination therapy Increase statin dose ‘Rule of ‘6%’ Statin + ezetimibe Statin + PCSK9 inhibitor Tolerability (statin + CETP inhibitor - future) Side effects
Summary • Recent evidence from clinical trials supports and emphasises the benefits of more aggressive LDL lowering in secondary prevention. • New guidelines reinforce previous treatment goals for very high risk, high risk and low to moderate risk categories of patients. • Treatment gaps persist linked possibly to perceived tolerability of statins and discontinuity of care. Optional therapeutic strategies can be adopted.
Recommend





More recommend
Explore More Topics
Stay informed with curated content and fresh updates.