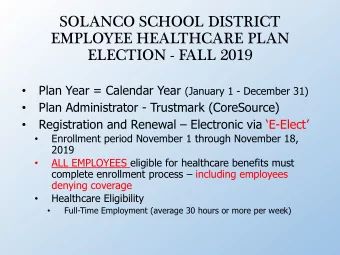
SOLANCO SCHOOL DISTRICT EMPLOYEE HEALTHCARE PLAN ELECTION - FALL 2018 Plan Year = Calendar Year (January 1 - December 31) • Plan Administrator - CoreSource • Registration and Renewal – Electronic via ‘E - Elect’ • Enrollment period October 31 through November 19, • 2018 ALL EMPLOYEES eligible for healthcare benefits must • complete enrollment process – including employees denying coverage Healthcare Eligibility • Full-Time Employment (average 30 hours or more per week) •
PLAN ELECTIONS • Preferred Provider (PPO) • Deductibles • Preferred Providers - $500/Individual or $1,500/Family • Non-preferred Providers - $1,000/Individual or $3,000/Family • Qualified High Deductible Healthcare Plan (HDHP) • Deductibles • Preferred Providers - $2,000/Individual or $4,000/Family • Non-preferred Providers - $4,000/Individual or $8,000/Family • Long-Term Substitutes not eligible for HDHP • Hires after April 1 not eligible for HDHP until following plan year • Identical Medical Coverage • Different Deductibles/Co-Pays
PPO PLAN • Employee responsible for all medical and RX costs until deductible satisfied • Each family member must satisfy individual deductible until overall family deductible satisfied • Employee/member responsible for co-pays • Employee may contribute to Flexible Spending Account (FSA) • Exception: Spouse participates in HDHP & contributes to HSA
PPO Plan Deductibles and Co-pays No Changes from 2018 2015 2016 2017 2018 2019 Deductibles 200/600 300/900 400/1000 500/1500 500/1500 Co-Pays: Physician $ 35.00 $ 35.00 $ 35.00 $ 35.00 $ 35.00 Specialist $ 45.00 $ 45.00 $ 45.00 $ 45.00 $ 45.00 ER $ 50.00 $ 75.00 $ 75.00 $ 100.00 $ 100.00 Chiropractic $ 25.00 $ 25.00 $ 25.00 $ 30.00 $ 30.00 Urgent Care $ 35.00 $ 35.00 $ 35.00 $ 40.00 $ 40.00 RX: Generic $ 10.00 $ 10.00 $ 10.00 $ 10.00 $ 10.00 Brand $ 30.00 $ 30.00 $ 30.00 $ 30.00 $ 30.00 Non-Formulary 50% to $75 50% to $75 50% to $75 50% to $75 50% to $75 Specialty N/A $ 75.00 $ 75.00 $ 100.00 $ 100.00 4
HDHP • Employee responsible for all costs until deductible satisfied • Overall plan deductible must be satisfied • Total $ deductible regardless of individual • Office visit co-pays waived until deductible satisfied • Collected by many medical offices - applied against deductible • Health Savings Account (HSA)
HSA • School District Contributions • HSA contributions permitted to maximum IRS limit (employer + employee) • 2019: Individuals - $3,500, Family - $7,000, Age 55+ Catch-up additional $1,000 • Contributions income tax exempt (Federal, State, Local) SLC – 35% or more tax savings • Employee owned bank account • Pay current or future qualified medical expenses • Refer to IRS Publication 502 • HSA distribution may not apply against deductible
HSA Contributions - Front Load Employee Account ***"Cohort" Employee only Employee Contributions to H S A for Tier- Solanco Total Paid To Premium Active Employees only Contributes H S A 2018 Max** 2019 Max** Contributes* District Yr. 1 1,600 500 2,100 3,450 3,500 2,000 District Yr. 2 1,500 500 District Yr. 3 1,250 500 1,750 Deductible is : $ 2,000.00 Family Tier_ Employee Total Paid To Solanco Premium H S A 2018 Max** 2019 Max** Contributes Contributes* District Yr. 1 3,200 1,000 4,200 6,900 7,000 District Yr. 2 3,000 1,000 4,000 District Yr. 3 2,500 1,000 3,500 Deductible is : $ 4,000.00 * Employee = Employee share is the required amount, it is flowing from the Employees required Premium Share each employee is paying as per the CBA. These funds are collected by the district (as district funds) and returned to the Employee H S A account. **Maximum Excludes additional $1,000 an Employee can contribute in the year turning age 55 or if age 55 or older. *** Cohort means the "year" you elect in to the HDHCP. The yearly amounts require an employee to be 'in' the "Q" plan for the entire year. (IRS annual amounts are pro-rated if not completing an entire year) For year one, payments are paid in January to get the employee started. Years thereafter are paid in January and September at 65/35% ratio, and the employee must be actively employed to receive the second payment. 33
HSA (Continued) • HEALTHEQUITY Administers HSA • VISA health account debit card • Investment income tax exempt • Investment options • Employee controlled or advisor managed • 20% Penalty on Non-Medical disbursements • Penalty waived after age 65 – Disbursement taxed as ordinary income • IRS Form1099-SA issued to employee • Employee complete IRS form 8889 • HSA governed by IRS regulations - Obey Rules
HSA How To: Doctors Visits • No co-pays billed until deductible satisfied 1 Go to the doctor • CoreSource adjusts price based on discounts Doctor sends insurance 2 • Pay doctor from HSA funds, if carrier the bill funds are available. Pay out of Claim integrated pocket if funds aren’t available and 3 into member portal reimburse yourself later or not. • NOTE: Who Pays or where funds come from ---Physician or Health care provider DOES NOT MATTER....You choose HOW/what account to pay from . *This card is issued by The Bancorp Bank pursuant to a license from Visa U.S.A. Inc. The Bancorp Bank; Member FDIC.
Member HSAExperience Medical Claims If deductible has not been met, provider Member goes will bill to Doctor, shows member for CoreSource card Member pays their plan outstanding When the negotiated provider bill member has portion. using funds claim activity, on HSA card an EOB from or personal If deductible CoreSource is daily daily has been met, funds through sent for each CoreSource plan will pay member claim. Claim Doctor sends visit sends claims to details andcoding provider for portal information and HealthEquityfor to CoreSource/ESI service. If monthly record keeping for claims member owes statements on andmember adjudication coinsurance, HSA funds and portal provider will bill account population member for information is their portion. available on daily HealthEquity portal.
HSA How T o Pharmacy Prescriptions 1 Show your CoreSource Express Scripts Card Go to pharmacy (ESI) card Pharmacy 2 applies discount Pay with your HSA card Or Cash or other ? Pharmacy sends claim to 3 insurance carrier Insurance carrier applies amount to your deductible — no paperwork needed *This card is issued by The Bancorp Bank pursuant to a license from Visa U.S.A. Inc. The Bancorp Bank; Member FDIC. 11
HSA Member Experience Pharmacy Claims Member goes to Pharmacy and shows daily CoreSource/ESIcard When the member has claim activity, they will receive an EOB from ESI for each claim. Claim information and Pharmacyand daily monthly statements on HSA card send HSA funds and account Pharmacy verifies payment eligibility. information is available information to on each member’s ESI If out of pocket max immediate HealthEquityportal. HealthEquity is not met, member for record can pay using HSA keeping and card or out of pocket. account tracking. 12
PREVENTIVE CARE Both PPO and HDHP cover In-Network Preventive Care, Screenings, Immunizations at 100% - (No Co-Pays, Deductible Not Applicable) • Periodic health evaluations (e.g., annual physicals) • Screening services (e.g., mammogram, pap test, colonoscopy) • Routine pre-natal and well-child care • Child and adult immunizations • Tobacco cessation programs • Obesity weight loss programs 13
PENDING E-ELECT COMMUNICATION • Be alert for email issued from SolancoBenefitElections@coresource.com • Worksheet attachment • Encrypted worksheet password is: ‘employee’s home address zip code’ • Worksheet contains link to www.eelect.com • Follow worksheet instructions to complete enrollment
Worksheet Attachment
HEALTHCARE PLAN PREMIUMS 24 - PAY EMPLOYEE EMPLOYEE + 1 FAMILY EMPLOYEES ONLY ANNUAL $9,614.28 $15,382.80 $22,112.76 PREMIUM EMPLOYEE SHARE 8.0% 9.0% 10.0% MONTHLY $801.19 $1,281.90 $1,842.73 PREMIUM PER PAY $32.05 $57.69 $92.14 DEDUCTION EMPLOYEE SHARE 6.0% 7.0% 8.0% WELLNESS PROGRAM REDUCTION – 2% WELLNESS PER PAY $24.04 $44.87 $73.71 DEDUCTION
WELLNESS PROGRAM REDUCTION 24 - PAY EMPLOYEE EMPLOYEE + 1 FAMILY EMPLOYEES ONLY WELLNESS PER PAY PREMIUM $8.01 $12.82 $18.43 REDUCTION ANNUAL WELLNESS $192.24 $307.68 $442.32 PREMIUM REDUCTION EMPLOYEE/SPOUSE MUST COMPLETE BIOMETRIC SCREENINGS AND FLU SHOT DURING 2018 (OR SUBMIT APPROPRIATE DOCUMENTATION FROM PHYSICIAN) TO RECEIVE 2019 HEALTHCARE PREMIUM REDUCTION
HEALTHCARE PLAN PREMIUMS 19 - PAY EMPLOYEE EMPLOYEE + 1 FAMILY EMPLOYEES ONLY ANNUAL $9,614.28 $15,382.80 $22,112.76 PREMIUM EMPLOYEE SHARE 8.0% 9.0% 10.0% MONTHLY $801.19 $1,281.90 $1,842.73 PREMIUM PER PAY $40.48 $72.87 $116.38 DEDUCTION EMPLOYEE SHARE 6.0% 7.0% 8.0% WELLNESS PROGRAM REDUCTION – 2% WELLNESS PER PAY $30.36 $56.67 $93.11 DEDUCTION
WELLNESS PROGRAM REDUCTION 19 - PAY EMPLOYEE EMPLOYEE + 1 FAMILY EMPLOYEES ONLY WELLNESS PROGRAM PER $10.12 $16.20 $23.27 PAY REDUCTION ANNUAL WELLNESS $192.24 $307.68 $442.32 PROGRAM REDUCTION EMPLOYEE MUST COMPLETE BIOMETRIC SCREENINGS AND FLU SHOT DURING 2018 (OR SUBMIT APPROPRIATE DOCUMENTATION FROM PHYSICIAN) TO RECEIVE 2019 HEALTHCARE PREMIUM REDUCTION
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries