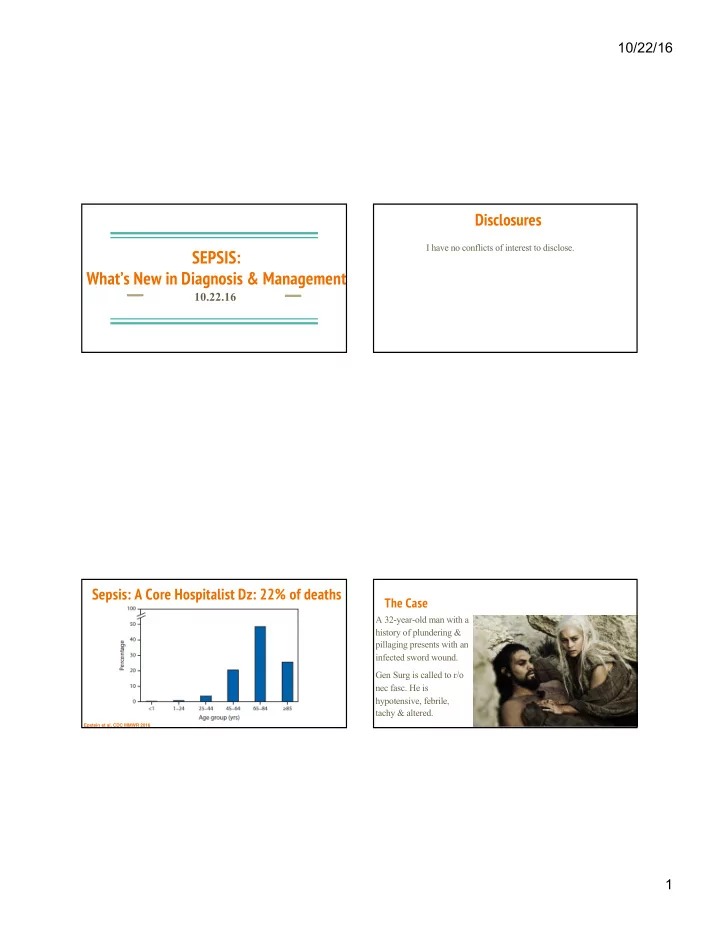
10/22/16 Disclosures I have no conflicts of interest to disclose. SEPSIS: What’s New in Diagnosis & Management 10.22.16 Sepsis: A Core Hospitalist Dz: 22% of deaths The Case A 32-year-old man with a history of plundering & pillaging presents with an infected sword wound. Gen Surg is called to r/o nec fasc. He is hypotensive, febrile, tachy & altered. Epstein et al, CDC MMWR 2016 1
10/22/16 How To Approach the Septic Patient Sepsis: What’s New i. Dx of Sepsis (Old & New!) in Diagnosis & ii. Phases of Sepsis Management Management iii. 2016 Evidence-Based Sepsis Updates Our Roadmap for Today Burns How Did We Use to Define Sepsis? Trauma § Severity is on a spectrum SEPSIS § SIRS criteria: HR > 90, RR > 20 or PaCO2 < 32, WBC > 12 or < 4 or SEVERE INFECTION SIRS > 10 % bands, T > 38 or < 36 SEPSIS § Severe Sepsis = SIRS + Acute Organ Dysfunction § Septic Shock = Severe Sepsis + hypotension not reversed w/ IVF Pancreatitis § Multi-system Organ Failure (MSOF) Tox 2
10/22/16 What Represents Acute Organ Dysfunction? If It Ain’t Broke, Why Fix It? § Hypotension - SBP < 90 § 19-member task force by SCCM & § Hypoxemia European Society of Intensive Care Medicine § UOP < 0.5 mL/kg-hr § Definitions last revised in 2001 § INR > 1.5 § Non-specificity of SIRS criteria & § Plt < 100k patients with SIRS “at baseline” § Total Bilirubin > 4 § New research w/ better correlations § Lactate > 2 with clinical outcomes § New Altered Mental Status From: The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) But What About that Weird SOFA Thing? JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 New! But Improved? Table Title: Sequential [Sepsis-Related] Organ Failure Assessment Score a Singer et al, JAMA 2016 3
10/22/16 Simplifying SOFA & SEPSIS-3 How do we tell if Khal Drogo Has Sepsis? A. Check SIRS B. Check a SOFA C. Check qSOFA D. It depends on where he is . . . H ypotension A ltered mental status T achypnea 4
10/22/16 Difference Between The Sepses (?) How the Founders Intended Its Use . . . Singer et al, JAMA 2016 Power of Δ SOFA Show me the Data! § 12% of ICU patients have 0 SIRS § ΔSOFA from HD1 to HD3 criteria § If you get sicker . . . § In ICU patients with suspected infection, SOFA (AUROC = 0.74; 95% CI, 0.73-0.76) was superior to SIRS (AUROC = 0.64) for predicting hospital mortality § AUROC ~ Email spam filter Jones et al, Crit Care Med 2009 Kaukonen et al, NEJM 2015 5
10/22/16 Most Powerful Statement. Take Home Points: Dx of Sepsis § Sepsis-3 defined new diagnostic criteria but uses TBD . . . “Patients with a SOFA score of 2 or § Remember qSOFA (BP, AMS, Tachypnea) in non-ICU more had an overall mortality risk of approximately 10% in a general hospital § SOFA score helps prognosticate mortality in ICU – ΔSOFA > 2? population with presumed infection. This is greater than the overall § No more severe sepsis in the new criteria but still think of organ dysfunction mortality rate of 8.1% for ST-segment elevation myocardial infarction.” § Not yet endorsed by ATS, ACEP, Medicare, and more . . . Phase 1 (Hours 0 – 6): Early Dx & Proactive Stabilization Sepsis: What’s New i. Dx of Sepsis (Old & New!) q Early recognition (with our detection tools) in Diagnosis & ii. Phases of Sepsis q Adjunctive diagnostic measures (such as lactate) Management Management q Early IV fluids iii. 2016 Evidence-Based Sepsis Updates Our Roadmap for Today q Early broad-spectrum antibiotics q Vasopressors if unresponsive to fluids q Central access if you need vasopressors 6
10/22/16 Sepsis Presents Atypically! Initial Lactate Level & 28-day Mortality q Elderly 28-day mortality (%) 50 40 q ESRD on HD 30 20 q HIV 10 0 Non-Shock Shock q Immunocompromised Low 8.7 15.4 Intermediate 16.4 37.3 q Transplant pts High 31.8 46.9 Mikkelsen et al, Crit Care Med 2009 7
10/22/16 “Dynamic Empiricism” and our EMR DDx: Dr. Jen Babik’s Head-to-Toe Approach Phase 2 (Hours 6-24): Finding the Source of Sepsis •Osteomyelitis q It all starts with a careful history & physical! •Nosocomial meningitis CNS MSK •Septic arthritis (post-NSG) •Gout q Consider blood, urine, sputum, stool cx (depending) •Nosocomial Sinusitis •Cellulitis at line sites HEENT •Hospital-acquired URI Skin •Infected decub ulcer •Surgical site infection •Hospital-acquired PNA q Always do basic imaging (CXR, bedside U/S/TTE) •CRBSI Pulmonary •Empyema Bloodstream •Candidemia •ARDS q Consider advanced imaging (CT Head, Abdomen/Pelvis, Lower •Drug Fever •Endocarditis Cardiac •Central fever •Pericarditis •DVT/PE Extremities) • C. Difficile Other non- •Malignancy •CA-UTI infectious •Rheumatologic •Abdominal abscess etiologies •Post-op fever q Consider advanced dx procedures (LP, bronch, etc) GI/GU •Peritonitis •Transfusion reaction •Acalculous cholecystitis •Transplant rejection •Pancreatitis •Adrenal insufficiency 8
10/22/16 ALWAYS Consider Mimics of Septic Shock! What Might Khal Drogo Have Besides Sepsis? q Cardiac Tamponade Cardiogenic shock A. Cardiogenic shock q q Acute valvular dysfxn Hypovolemia/Blood loss B. Hypovolemic shock q q Aortic Dissection Pulmonary embolism C. Acute liver failure q q Anaphylaxis Myxedema coma D. Aortic dissection q q Adrenal crisis Toxidromes E. All of the Above q q HLH Acute liver failure q q And more! Phase 3 (1-3d): Narrowing Focus, Limiting Iatrogenesis q Narrow Abx based on cx data (esp Vanco!) q Consider diuresis to counteract your flooding q Limit ICU Harms: PT/OT, Delirium, De-Line q Recognize differing trajectories of illness Skrupsky et al, Anesthesiology 2011 9
10/22/16 Take Home Points: Rx of Sepsis Sepsis: What’s New i. Dx of Sepsis (Old & New!) § Early diagnostics (including lactate) & resuscitation matter in Diagnosis & ii. Phases of Sepsis § Hunt aggressively for the source – step-wise approach Management Management iii. 2016 Evidence-Based Sepsis § Think head-to-toe and consider septic shock mimics Updates Our Roadmap for Today § Harness the power of the EHR to identify sepsis, but remember limitations § Recognize different clinical trajectories of sepsis Graveyard of Missed Deadlines But What About that Weird SOFA Thing? 10
10/22/16 The “Old” Way Graveyard of Sepsis Therapies § RCT of early goal directed therapy (EGDT) versus standard XIGRIS of care EGDT ‘ROIDS § Mortality was primary outcome § There was a 15% absolute risk reduction in mortality § Issues: Conflict-of-interest, heavy ED influence, high baseline mortality, & many more! “New” Era: ProCESS, ARISE & ProMISe “New” Era: ProCESS, ARISE & ProMISe § No significant difference in the 90-day mortality between the EGDT and usual care groups (29.5% vs 29.2%, p=0.90), despite EGDT having (in first 6 hours): u Higher rate of vasopressors u More RBC transfusions u More IVF fluids ProMISE, NEJM 2015 ARISE, NEJM 2014 11
10/22/16 “New” Era: ProCESS, ARISE & ProMISe Take Home Points from This Trifecta § Strict protocol for EGDT did not lead to improved outcomes § Increased costs with EGDT protocol § All patients basically got Abx + 2 L IVF pre-randomization, suggesting usual care has changed since Rivers § Only 50% got central lines in usual care group ProCESS, NEJM 2014 Do Steroids Work For Septic Shock? (Redux) Levosimendan for Septic Shock § Randomized patients to § LeoPARDS RCT double continuous infusion of 200 blind placebo-controlled mg of hydrocortisone for 5 trial of this Ca-sensitizer days + taper to d11 vs § Not currently licensed in placebo the USA § Goal was to prevent severe § No difference in mean sepsis à septic shock SOFA score or mortality Keh et al, JAMA 2016 Gordon et al, NEJM 2016 12
10/22/16 Graveyard of Sepsis Therapies Under-the-Radar Trial: Tylenol for Fever in the ICU § Well-designed RCT! XIGRIS EGDT § No reduction in ‘ROIDS mortality or LOS § Trial was of IV Tylenol, of note § Treat for comfort Young et al, NEJM 2015 Which Tool Will Best Predict His Response to Fluids? Will My Hemodynamically Unstable Pt Respond to IVF? § Passive leg raise vs CVP vs A-line PPV vs IVC U/S A. Passive Leg Raise § No reduction in mortality or LOS B. CVP § Trial was of IV Tylenol, of note C. A-line PPV § Treat for comfort D. IVC U/S E. None of the above Bentzer et al, JAMA 2016 13
10/22/16 Take Home Points: New Trials Procalcitonin Testing in the ICU § Retrospective study of matched 1:3 cases (~33K:99K) pts w/ ICU day 1 PCT testing vs § More trials for the sepsis graveyard – EGDT, steroids no PCT testing § Decreased hospital LOS, ICU LOS, lower § Treat fevers in the ICU for comfort hospital costs, lower Abx days § Some high-tech (procalcitonin) & low-tech (leg raise) dx for § No mortality difference sepsis § $81 per test difference in cost § More literature on sepsis management controversies Balk et al, Chest 2016 Sepsis: What’s New i. Dx of Sepsis (Old & New!) in Diagnosis & ii. Phases of Sepsis Management Thank You! Questions? Management iii. 2016 Evidence-Based Sepsis Updates Lekshmi.Santhosh@ucsf.edu Our Roadmap for Today 14
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries