Robert E. Ratner, MD Chief Scientific and Medical Chief Scientific - PDF document
Robert E. Ratner, MD Chief Scientific and Medical Chief Scientific and Medical Officer Normal Threshold Plasma Glucose Levels for Activation of Counterregulation and Symptoms B: Neuroglycopenic B: Neuroglycopenic A: Autonomic symptoms A:
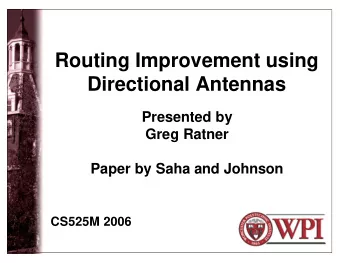
Robert E. Ratner, MD Chief Scientific and Medical Chief Scientific and Medical Officer Normal Threshold Plasma Glucose Levels for Activation of Counterregulation and Symptoms B: Neuroglycopenic B: Neuroglycopenic A: Autonomic symptoms A: Autonomic symptoms C: Cognitive dysfunction C: Cognitive dysfunction symptoms symptoms C B A Suppression of Insulin Secretion Growth Hormone Pancreatic Polypeptide Epinephrine Glucagon Glucagon Cortisol Norepinephrine 30 40 50 60 70 80 90 Glycemic Threshold (arterial glucose, mg/dL) 1
Risk Factors for Severe Hypoglycemia Low HbA 1c 1c Factors interfering with counterregulation Increases of insulin sensitivity Changes in drug metabolism Inadequate nutrition I d t t iti Other medical conditions (e.g., impaired cognition) How Often Does Hypoglycemia Occur in Diabetes? Daily to about 1/wk 100 1/mo to several times/mo / / 90 90 % equency of NSHE, % 80 Only a few times/y or very rarely 70 64.5 60 50 40.2 40 34.9 30 24.9 23.5 20 20 12 12 Fre 10 0 T1DM T2DM NSHE, nonsevere hypoglycemic events. Survey 409 US patients with T1DM (n = 200) and with T2DM (n = 209). Brod M, et al. Value Health . 2011;14:665-671. 2
When Does Hypoglycemia Occur With Diabetes? Awake and at work Awake but not at work 20% During sleep at night 30% 50% 50% 1/5 of all nonsevere hypoglycemia occurs nocturnally NSHE, nonsevere hypoglycemic events. Survey 409 US patients with T1DM (n = 200) and with T2DM (n = 209). Brod M, et al. Value Health . 2011;14:665-671. All Hypoglycemia Negatively Affects Quality of Life in Patients With T2DM Alvarez-Guisasola 1 Marrett 2 (N = 1709; 38% with (N = 1984; 63% with events) events) 0 0 0 0 0 0 RQoL Decrement RQoL Decrement − 0.01 -0.05 -5 − 2.68 a − 0.06 -0.1 a − 6.42 -10 a -0.15 − 0.13 -15 a -0.2 − 16.09 -20 a − 0.21 -0.25 -25 a HR HR Hypoglycemia Severity Hypoglycemia Severity Hypoglycemia is also associated with lower treatment satisfaction, poorer adherence, and greater resource utlization 3 1. Alvarez-Guisasola F, et al. Health Qual Life Outcomes . 2010;8:86. 2. Marrett E, et al. BMC Res Notes . 2011;4:251. a P < .05 vs no reported hypoglycemia. 3. Williams S, et al. Diabetes Res Clin Pract . 2011;91:363-370. 3
Severe Hypoglycemia Is Associated With Increased Risk of Mortality and CV Events Macrovascular events ADVANCE Trial Results 1 3.45 (2.34-5.08); P < .001 Death—any cause 3.30 (2.31 4.72); P 3.30 (2.31-4.72); P < .001 .001 Death—CV cause 3.78 (2.34-6.11); P < .001 Death—non-CV cause 2.86 (1.67-4.90); P < .001 Macrovascular 0.1 1 10 events 1.88 (1.03-3.34); P = .04 VADT Results 2 Death—any cause 6.37 (2.57 15.79); P 6.37 (2.57-15.79); P = .0001 Death—CV cause 3.73 (1.34-10.36); P = .0117 0.1 1 10 Decreased Risk Increased Risk Hazard Ratio (95% CI) 1. Zoungas S, et al; ADVANCE Collaborative Group. N Engl J Med . 2010;363:1410-1418. 2. Duckworth W, et al; VADT Investigators. VA Diabetes Trial (VADT) update. ADA 70th Scientific Sessions. 2010: http://webcasts.prous.com/netadmin/webcast_viewer/Preview.aspx?type=0&lid=9473&pv=2&preview=False&idcl=0. Hypoglycemia, by Age 200 65-74 180 180 75-84 160 Rate per 152 ≥ 85 126 141 140 100,000 Patient-Years 120 121 100 80 72 70 70 60 60 40 20 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 Year 8 4
Hospitalization for Hyperglycemia and Hypoglycemia 140 130 114 114 120 105 Rate per 100 100,000 94 Patient-Years 80 70 60 40 Hyperglycemia Hyperglycemia 20 Hypoglycemia 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 Year 9 Adjusted for Diabetes Prevalence 900 820 800 800 700 Rate per 100,000 676 612 600 Patient-Years with Diabetes 500 400 300 367 200 200 Hyperglycemia 100 Hypoglycemia 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 Year 10 5
Hypoglycemia Hospitalizations as % of All-Cause T1DM and T2DM Hospitalizations 7.0% 6.4% 6.0% 5.0% 4.0% 3.4% 3.0% 2.0% 1.0% 0.0% T1DM T2DM Length of Stay T1DM patients with hypoglycemia stayed longer compared to those with all-cause hospitalizations 8 7 2 7.2 7 All-cause Hospitalizations of stay in days 6 5.0 5 4.6 Type 1 Diabetes hospitalizations 4 length of stay length of stay Length o 3 Hypoglycemia 2 Hospitalizations in Type 1 Diabetes 1 0 6
Charges for Hospitalizations with Hypoglycemia in T1DM (US$ per admission) $60,000 $46 039 $46,039 $50,000 $40,000 $33,564 $30,655 Charges $30,000 $20,000 $20,000 $10,000 $0 Hypoglycemia in T1DM T1DM All-Cause Hospitalizations National Bill : Total Charges for Hypoglycemia Hospitalizations in T1DM Total hospitalizations = 20,839 (95% CI = 19,233 - 22,445) Charge per hospitalization = $46,039 (CI = $42,144-$49,934) Ch h it li ti $46 039 (CI $42 144 $49 934) Total charges = $ 959,406,721 As a comparison, hypoglycemia hospitalizations in T2DM : Total hospitalizations = 248,422 (CI = 234,321-262,523) Charges per hospitalization = $48,569 (CI = $45,781- Ch h it li ti $48 569 (CI $45 781 $51,357) Total charges = $ 12.07 billion Average Charge of US All-Cause Hospitalization: $33,232 7
Recommend






More recommend
Explore More Topics
Stay informed with curated content and fresh updates.