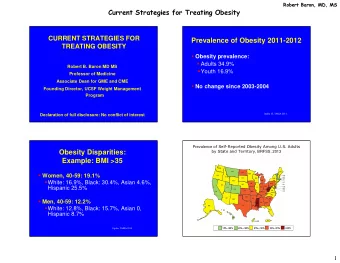
Prevalence: Adults (Boston) Survey: N = 28,176 Results - PDF document
GENDER NON-CONFORMING / TRANSGENDER YOUTH: CURRENT CONCEPTS, MANAGEMENT, & BARRIERS TO CARE Stephen M. Rosenthal, M.D. Professor of Pediatrics Em. Program Director, Pediatric Endocrinology Medical Director, Child & Adolescent Gender
GENDER NON-CONFORMING / TRANSGENDER YOUTH: CURRENT CONCEPTS, MANAGEMENT, & BARRIERS TO CARE Stephen M. Rosenthal, M.D. Professor of Pediatrics Em. Program Director, Pediatric Endocrinology Medical Director, Child & Adolescent Gender Center University of California, San Francisco Stephen.Rosenthal@ucsf.edu DISCLOSURE • No relevant financial relationships with a commercial interest to disclose • All Rx to be discussed: “Off-label” for Gender Dysphoric Youth Stephen M. Rosenthal, M.D. Professor of Pediatrics Em. Program Director, Pediatric Endocrinology Medical Director, Child & Adolescent Gender Center University of California, San Francisco 1
Thank You! OBJECTIVES: • Review epidemiology; mental health concerns • Review evidence for biologic underpinnings of gender identity • Review outcomes of current treatment model • Understand gaps in knowledge, barriers to care, priorities for research 2
How Common is Transgender? • Prevalence: Adults (Boston) – Survey: N = 28,176 – Results » Self-identified as Transgender » N = 131 » 0.5% Conron KJ et al. Am J Public Health, 2012 How Common is Transgender? • Prevalence in Youth – Not yet known • Our clinical program: – > 350 patients (1 st pt 2009) – 8-10 new referrals / month 3
Transgender Adolescents/ Young Adults: Mental Health Concerns • N = 360 (Boston) 180 transgender, 180 cisgender • Age: 12-29 yr (Avg. 19.6 yr) • Results: 2-3 x é é Risk (all p < 0.05) – Depression – Anxiety Disorder – Suicidal Ideation – Suicide attempt – Self-harm without lethal intent Reisner SL et al., J Adolesc people’s participant’s Health 56:274-279, 2015 “high esteem” one’s “not supportive” “strongly supportive” IMPACT OF PARENTAL SUPPORT “out” FOR TRANSGENDER YOUTH “very supportive” “somewhat supportive” “not very” “not all”, “not supportive” Figure 2. Proportion of trans youth age 16-24 years in Ontario experiencing negative health and life conditions, by level of parental support Parent(s) very supportive one’s Parent(s) somewhat to not at all supportive youth’s 100 90 80 70 60 50 N = 84 Youth 40 75 70 one’s 30 57 youth’s 20 34 10 23 4 0 “how Depressive Considered Suicide attempt, general?” symptoms* suicide, past yr past yr* * = statistically significant difference (p < 0.05) Travers R et al. Children’s Aid Society of Toronto & Delisle Youth Services, 2012 4
A ¡report ¡prepared ¡for ¡Children’s ¡Aid ¡ one’s IMPACT OF PARENTAL SUPPORT “trans” FOR TRANSGENDER YOUTH Figure 1. Proportion of trans youth age 16-24 years in Ontario experiencing positive health and life conditions, by level of parental support Parent(s) very supportive Parent(s) somewhat to not at all supportive 100 youth’s 90 80 70 60 50 100 92 40 82 N = 84 Youth 72 70 66 64 30 58 45 20 42 33 31 10 15 13 0 Satisfied with VG/excellent VG/excellent High self Intent to Adequate Adequate life* physical mental esteem* parent housing* food health health* * = statistically significant difference (p < 0.05) Travers R et al. Children’s Aid Society of Toronto & Delisle Youth Services, 2012 GENDER IDENTITY • Complex interplay • Biologic • Environmental • Cultural factors 5
EVIDENCE FOR BIOLOGIC UNDERPINNINGS OF GENDER IDENTITY • Insights from: • Genetics • Hormones • Brain • Not a “litmus test” of Transgender TRANSGENDER: ROLE OF GENETICS? • Twin Studies (Heylens G et al. J Sex Med 9:751-757, 2012) • Concordance for Gender Dysphoria • Comprehensive literature review • N = 23 monozygotic (8 F, 15 M) twin pairs • N = 21 same-sex dizygotic (5 F, 16 M) twin pairs • N = 7 opposite sex twin pairs • Results: Concordance for Gender Dysphoria • Monozygotic Twin pairs: 39.1% • Same-sex dizygotic twin pairs: 0% (p = 0.005 vs. MZ twins) • Opposite sex twin pairs: 0% • Studies of individual candidate genes: inconsistent 6
HORMONES & GENDER IDENTITY • Most transgender individuals do not have a “Disorder of Sex Development” (DSD) • Studies in patients with DSD – Informed our understanding of gender identity development – Role of prenatal/ (postnatal) androgens HORMONES & GENDER IDENTITY • Insights from: • Congenital Adrenal Hyperplasia (CAH) • 46 XY cloacal exstrophy 7
SEXUAL DIFFERENTIATION Role of DHT & Androgen Receptor DSD: 2 Extremes -- CAH (46XX) --Cloacal Exstrophy (46XY) CAH 46XX Female 8
Congenital Adrenal Hyperplasia (CAH) ( CYP21A2 Deficiency) • 46 XX raised Female (F) – N = 250 » 94.8 %: F gender identity » 5.2%: M gender or gender confusion » 10-20 x é é risk vs. control » No correlation with degree of genital virilization • Supports “some” role of prenatal androgens in gender development Dessens AB et al. Arch Sex Behav 2005 Cloacal Exstrophy • N = 16 46XY Males – 14 underwent neonatal sex reassignment to female • Follow-up: age 5-16 yr • Study – Parent questionnaires – Subjects’ stated Gender Identity • Outcome – 8/14 declared Male Gender » 4/8 before knowing birth status – 2/16 raised as male stayed male • Supports “some” role of prenatal androgens in gender development Reiner WG et al. N Engl J Med 350:333-341, 2004 9
Neurobiologic Basis for Transgender? • Dimorphic brain structures (human) • Sexually dimorphic – Cell groups preoptic & anterior hypothalamic areas » INAH-1,-2,-3 – Suprachiasmatic nucleus – Bed nucleus of the stria terminalis (BSTc) – Anterior commissure – Right putamen • Sexual orientation dimorphic – INAH-3 • Gender dimorphic? Neurobiologic Basis for Transgender? • Numerous Gray, White matter studies – Sexually dimorphic structures more closely aligned with gender identity than with physical sex – Seen even before cross-sex hormones are given Luders E et al. NeuroImage 46:904-907, 2009 Rametti G et al. J Psychiatric Research 45:199-204, 2011 Hoekzema E. et al. Psychoneuroendocrinology, 2015 10
Sex beyond the genitalia: The human brain mosaic • MRI • Multiple data sets (4): 1400 human brains • Assess degree of internal consistency • Voxel-based morphometry (VBM) • Focused on areas which show largest sex differences (least overlap between M, F) • Principal finding: • Variability more prevalent than internal consistency Joel D et al. PNAS, November 30, 2015 Anterior Hypothalamus: Evidence for “ Functional ” Gender Dimorphism • Positron Emission Tomography (PET) – Changes in regional blood flow – Smelling of 2 “odorous” compounds – Putative pheromones » Progesterone derivative of 4,16 androstadien-3-one (AND) » Human male sweat, saliva, semen » Estrogen-like compound (EST) » Urine of pregnant females Berglund H et al. Cerebral Cortex, 2008 11
Anterior Hypothalamus: Evidence for “ Functional ” Gender Dimorphism • Anterior Hypothalamus activated by AND, EST in “ sexually ” dimorphic manner – Females: activated by AND – Males: activated by EST • Study: – N = 12 MTF adults » Never-received hormonal Rx ! – N = 24 controls (12 M, 12 F) • Results: – MTFs: Ant hypothal activated by AND (F pattern) » Differed from Male controls (p < 0.05), not from Female controls Berglund H et al. Cerebral Cortex, 2008 12
What is the Natural History of Transgender/ Gender Dysphoria in Children & Adolescents? Children & Adolescents with GD: Natural History • Symptoms of Gender Dysphoria in pre-pubertal children ↓ or disappear in 70-95% of cases • Gender Dysphoria persisting into early puberty: • Likely transgender as adult! 13
Management of Adolescents with GD Current Practice: • Amsterdam VU University Med Ctr • Pubertal suppression with GnRH agonists (GnRHa) • Tanner 2 • Gender dysphoria from early childhood • ↑ Gender dysphoria with pubertal onset • Absence of psychiatric co-morbidity that might interfere with treatment • Adequate psychosocial support • Demonstrated understanding of process GnRH Agonists in Gender Dysphoric Youth: Expected Benefits • “Buys time” • Prevents experiencing puberty of undesired sex • Fully reversible! • Once puberty completed, can only be incompletely reversed-- Difficult to “blend” • MTF: Low voice, masculine facial & neck features in MTF • FTM: Breast development 14
Recommend









More recommend
Explore More Topics
Stay informed with curated content and fresh updates.