Practice placement – OCT 312 Learning Disabilities (LD) Specialist Health Team Case study presentation on a service user who has a mild LD and how this impacts on her role of parent Student number 10529913
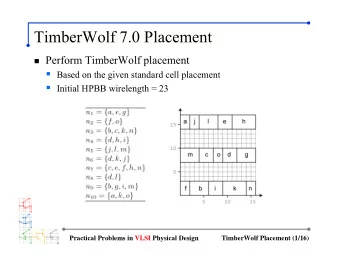
Learning Disability Specialist Team Placement setting/Role of occupational Occupational Therapy therapist Sensory Processing Daily Living Skills (ADLs) Dementia Behaviour That Challenges offer assessment and therapy Assessment · baseline assessment · Environmental evidence to gain greater understanding and follow up. based assessment · Sensory • Concern regarding skill loss of how an individual • Specific assessment and advice · Changing needs profile. processes sensory regarding individuals who may be assessment, e.g. · Understanding occupational information; Ayres SI therapy, on the dementia care pathway Assessment of changing needs, routine, consistency and when sensory integration is • Skills training/recommendations functional, social, structure. identified as a occupational environmental needs as · Staff support/training • Daily living skills assessment participation barrier when an individuals placement is dementia progresses, encouraging a MDT approach, - proactive approach with breaking down and little is staff support/training. systemic, family/carer carers to take forward a understood about their support - Identify changes to relationship work ‘sensory diet’; enabling the needs equipment needs, refer · Physical screening is part of individual to engage in on to social care initial LD OT assessment, • Placement suitability meaningful activities and • Supporting the role of parents Occupational where onward referral is reduce fluctuating arousal who have a learning disability. Therapist’s . identified where indicated. levels. [1] (Creek, 2003), [2] (Parker, 2011), [3] (Lillywhite & Haines, 2010), [4] (NLDPS, 2015).
The service user Mild learning Disability, Noonan Assessed to Syndrome, dual have capacity sensory and to consent impairment. to treatment. [1] [1] (Clipartbarn, 2017).
Governing body/Policies, guidelines and legislations Relevance to case study/impact on practice Royal College of Occupational Therapists (RCOT) Professional Standards [14]. Service provision, patient welfare, professionalism and ethical frameworks within which registrants must Royal College of Occupational Therapists (RCOT) Code of work. ethics and professional conduct [1]. Healthcare Professional's Council (HCPC) Standards of conduct, performance and ethics [2]. Management of Noonan Syndrome – A Clinical Guidance Guidelines recommend people with diagnosis of Noonan’s Syndrome are helped to access support for National Policy Drivers [3]. employment, independent living and social skill interventions as needed [3]. Equality Act - Reasonable adjustments [4]. The act ensures, as far as possible, by reasonable means that a person with a disability experiences the least Policies and Legislations disadvantage. Must ensure reasonable adjustments are made to service users to ensure practice is person- centred and each person is given sufficient opportunity to understand and engage.; ensures all correspondence Kelly receives is an accessible format [13]. Mental Capacity Act [5]. Complying with act is important as it enables people with a LD to make choices, empowering them to make informed decisions and to set their own goals to improve their quality of life. SCIE – helping people with LD in their parenting role [6.] This resource has not been updated since February 2005. It may not reflect current policy but still provides valuable practice guidance; summary of potential support parents with a LD may need. Care Act – Safeguarding [7]. People with a LD can be vulnerable and so it is essential, in practice to be able to identify abuse, develop safety plans and make alerts , to promote the wellbeing and safety of the service user [13]. National Institution of Care Excellence (NICE) - Encourage people with multimorbidity to clarify what is important to them, including their personal goals, Multimorbidity: clinical assessment and management [8]. values and priorities. These may include taking part in social activities and playing an active part in family life, maintaining their independence; further supports the need to work with Kelly to gain increased independence and be able to actively engage in her parenting role. Confidentiality, sharing of information, gaining consent. Consent and Capacity to consent policy[9]. Local Policy Drivers Guidance for safe practice in the correct handling of food; impacting on my own ability to be able safely and Food hygiene policy [10]. correctly handle food when working with Kelly. Within community working have to ensure personal safety when working alone Lone working [11]. [1] (RCOT, 2017a), [2] (HCPC, 2016), [3] (NSGDG, 2010). [4] (Equality Act, 2010), [5] (Mental Capacity Act, 2005), [6] )SCIE, 2005), [7] (Care Act, 2014), [8] (NICE, 2016), [9] (XXXX, 2015a), [10] (XXXX, 2015b), [11] (XXXX, 2016), [12] McSherry & Pearce, 2011), [13] (Lillywhite & Haines, 2010), [14] (RCOT, 2017b).
Learning disability [1] [2] A LD is defined as inclusion of the following criteria: initiated before adulthood, a significantly reduced ability to understand new or complex information to learn new skills; a reduced ability to cope independently having a lasting effect on development; with intellectual impairment being classified as an Intelligence Quotient (IQ) of 70 and below. Prevalence [8] End of March 2015 there were 252,446 people of all ages on LD registers. [7] Noonan Syndrome [3] Varying greatly in breadth and severity. It is common for those affected by Noonan Syndrome to have an array of physical and health problems, often causing an under development of hearing and speech. Epidemiology [3] Impact of condition on occupational performance ability and participation Learning Disability [6]. • Struggle to break down and process complexed information which could contribute to poor planning and sequencing which will ultimately affect engagement and participation in occupation Dual sensory loss (Possibly secondary to Noonan Syndrome) [4][5] • diminishes communication and well-being and can cause social isolation, reduced independence, and cognitive impairment, impacting on an Kelly’s ability to access information and advice around health and wellbeing; resulting in difficulties with, maintaining social relationships and having a healthy lifestyle. Collectively, both can affect Kelly’s ability to communicate effectively and engage in her environment; limiting participation in occupations and so the demands of the activity will need to change in order to reduce the risk of occupational deprivation occurring, giving reason for referral to occupational therapy [6][9]. [1] (DOH, 2001), [2] (Holland, 2011), [3] ] (NSGDG, 2010), [4] (Sense, 2017), [5] (Schneider et al., 2011), [6] (Lillywhite & Haines, 2010), [7] (Political Correctness and People with Disabilities, 2017), [8] (PHE, 2016), [9] (Hurst, 2009).
Kelly’s motivation for occupation -Volition • Does not work currently but has previously attended college and completed a Volition Habituation cookery class. • Recently, has not been able to engage in many meaningful occupations; • Reported to have an active interest in swimming. Kelly’s occupation organisation - Habituation Roles MOHO [1][2] – Information gathering • Parent, partner, friend, daughter. Performance Routines Environment • Caring for her son, parent and toddler group every Thursday afternoon – no skills formal structure. People with learning disabilities may be predisposed to Environment (facilitators and barriers to engagement in occupation) Physical environment – occupational alienation as a result of an inherent need • struggles to operate physical resources in home environment due to visual for ongoing support in at least one major life activity impairment. across multiple environments [5][6]; at risk if they are • Moved house – all level, accessible flat. not afforded meaningful choices and opportunities for Social environment – enriching occupational experiences by being supported • Partners mum very supportive of Kelly. to participate in occupations [3][4]. • Struggles in new social situations. • Relationship with partner. Therefore, important to use MOHO as a framework to • Receives support from sensory loss worker once a week – no evidence of care guide practice as it will be able to look at a persons planning. facilitators and inhibitors to occupational performance and participation [2]. The model allowed me to keep this focus in my Kelly’s occupation performance - Performance capacity assessment and treatment and to give a client centered • Struggling with some ADLs - mainly meal preparation and cooking. Reported to be independent in self care for both herself and her son. approach [1][2]. • Mild LD. • Noonan’s Syndrome; visual impairment, mixed conductive and sensorineural deafness secondary to Noonan’s syndrome. [1](Kielhofner, 2008), [2] (Lillywhite & Haines, 2010), [3] (Townsend & Wilcock, 2004), [4] (Mahoney et al ., 2016), [5](American Psychiatric Association, 2013), [6] (Wilcock & Hocking, 2015).
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries