
Practical Approaches to the Treatment of Obesity March 11, 2012 - PowerPoint PPT Presentation
Practical Approaches to the Treatment of Obesity March 11, 2012 David C.W. Lau, MD, PhD, FRCPC Depts. of Medicine, Biochemistry & Molecular Biology and Cardiac Sciences Julia McFarlane Diabetes Research Centre University of Calgary
Practical Approaches to the Treatment of Obesity March 11, 2012 David C.W. Lau, MD, PhD, FRCPC Depts. of Medicine, Biochemistry & Molecular Biology and Cardiac Sciences Julia McFarlane Diabetes Research Centre University of Calgary 403-220-2261 Email: dcwlau@ucalgary.ca
Disclosures • Research funding: Can Inst Health Research, AHFMR, Alberta Cancer Board, CDA, AstraZeneca, BMS, Dainippon, Eli Lilly, Novo Nordisk, Pfizer and sanofi-aventis • Consultant or advisory board member: Abbott, Allergan, Amgen, AstraZeneca, Bayer, Boehringer-Ingelheim, GSK, Eli Lilly, Merck, Novartis, Novo Nordisk, Pfizer, Roche, sanofi-aventis • Speaker bureau: CDA, HSFC, AstraZeneca, Abbott, Bayer, Boehringer- Ingelheim, Eli Lilly, GSK, Merck, Novo Nordisk, Pfizer sanofi-aventis and Sepracor
Objectives At the end of the presentation the participant will: 1. Understand the rationale for obesity management 2. Recognize the health benefits of modest weight loss 3. Incorporate health behaviour changes in the management of obesity and related cardiometabolic risks 4. Understand the role of pharmacotherapy and bariatric surgery 5. Overcome common barriers to successful weight management
Body Weight Classification by Body Mass Index (BMI) Weight (kg) BMI = Height (m 2 ) BMI (kg/m 2 ) Classification Risk of co-morbidities WC <102/88 >102/88 cm * Healthy wt 18.5-24.9 Normal Overweight 25.0-29.9 Increased High Obese Class I 30.0-34.9 High Very high Class II 35.0-39.9 Very High 40.0 Class III Extremely High * WC (waist circumference) cut-offs: >102 cm men and > 88 cm in women Canadian guidelines for body weight classification in adults. Ottawa: Health Canada; 2003
All-cause Mortality and BMI 64 57 prospective studies Overweight N = 894,576 Male 32 Annual deaths Female per 1000 16 & 95% CI (floated so matches PSC rate at ages 35-79) 8 4 15 20 25 30 35 40 50 Baseline BMI (kg/m 2 ) Prospective Studies Collaboration. Lancet 2009;373:1083-96
Mortality and BMI at Ages 35-79 Years Male Female 14 14 Vascular 12 12 Annual 10 10 deaths per 1000 8 8 Vascular 6 6 & 95% CI (floated so matches EU rate at Cancer (other ages 35-79) specified) Cancer (other 4 4 specified) Cancer (lung, mouth, Cancer (lung, pharynx, 2 2 mouth, larynx, oes.) Resp. pharynx, Respiratory larynx, oes.) 0 0 15 20 25 30 35 50 15 20 25 30 35 50 Baseline BMI (kg/m 2 ) Adjusted for age, smoking and study; 1 st 5 years of follow-up excluded Lancet 2009;373:1083-96
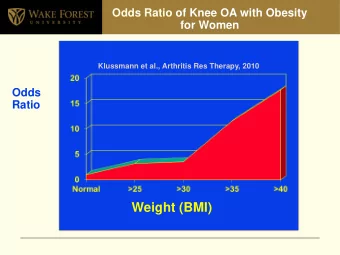
Medical Complications of Obesity Idiopathic Intracranial Pulmonary Disease Hypertension Stroke • Abnormal function Cataracts • Obstructive sleep apnea Coronary Heart Disease • Hypoventilation syndrome Diabetes Nonalcoholic Fatty Liver Hypertension Disease Dyslipidemia • Steatosis • Steatohepatitis Severe Pancreatitis • Cirrhosis Cancer Gall Bladder Disease Breast, uterus, cervix, colon, esophagus, pancreas, kidney, Gynecologic Abnormalities prostate • Abnormal menses Phlebitis • Infertility • Venous stasis • Polycystic ovarian syndrome Osteoarthritis Gout Skin
Obesity and Burden of Chronic Diseases • Overweight and obesity are attributable to the major comorbidities: 80% of Type 2 diabetes 32% of hypertension 30% of pulmonary embolism 27% of endometrial cancer Paeratakul S, et al. Int J Obesity 2002;26:1205-1261
The natural history of type 2 diabetes has changed because of obesity and can now occur 30 years earlier!
Global Prevalence of Overweight and Obesity in 1980 and 2008 9.1 million people from 199 countries Mean BMI in 2008 Men: 23·8 kg/m² (23·6-24·0) Women: 24·1 kg/m² (23·9-24·4) Average BMI of Canadian adults increased by 2 kg/m² to > 25 kg/m² (1981-2007)! Finucane MM, et al. Lancet 2011; 377:557-567
Recommendations on Classification • We recommend measuring BMI in all adults, and in children and adolescents (aged 2 years and older) [Grade A, Level 3] • Ethnic-specific values for overweight and obesity for people of South Asian or oriental descents: 23 kg/m 2 27 kg/m 2 Lau DCW, et al. Can Med Assoc J 2007;176 (8 suppl):S1-S13
Relationship between Glucose Factor and BMI Among South Asians (SA), Chinese (CH), Aboriginals (AP), and Europeans (EC) Razak F, et al. Circulation 2007; 115:2111-2118
INTER-HEART: 9 Modifiable RFs and MI Women Smoking Men Diabetes Hypertension Abdominal Obesity INTERHEART N=27,000 Psychosocial index 52 countries Fruits/Vegetables Exercise (-) Alcohol (-) Apo B / Apo AI Odds Ratio Yusuf S, et al. Lancet 2004;364:937-952
Waist Circumference Cut-points Cut Points Risk Factors Central obesity Men WC Women 94 cm (37 in) 80 cm (31.5 in) European, Mid-east 90 cm (35 in) 80 cm (31.5 in) S. Asians, Chinese For East Mediterranean, Middle East (Arab) and sub-Saharan African, use European cut-points For South and Central American and Japanese, use South Asian cut- points Adapted from Lau DCW, et al. Can Med Assoc J 2007;176 (8 suppl):S1-S13
Obesity Treatment Pyramid Obese Class 3 BMI 40 kg/m 2 Obese Class 2 BMI 35 kg/m 2 Obese Class 1 BMI 30 kg/m 2 Overweight BMI 25 kg/m 2
5 Principles That Every Health Care Provider Should Know 1. Obesity is a chronic condition which requires a long-term and sustainable treatment approach 2. Successful obesity management is about improving health and well-being, and not just weight loss 3. Early intervention means addressing root causes and removing barriers 4. Success is different for every individual 5. A person’s best weight may never be an ideal weight
1. Obesity is a chronic condition! • Obesity is a chronic and often progressive condition, not unlike diabetes or hypertension, and requires long-term management to prevent relapse • Successful management requires realistic and sustainable long-term treatment strategies • Short-term "quick-fix" solutions focusing on maximizing weight loss are unsustainable and associated with high rates of weight regain
2. Successful obesity management is about improving health and well-being • Obesity management is about improving health and well-being, and not simply losing weight and waist • Even modest body weight loss can lead to significant improvements in health and well- being in many people • Weight maintenance and prevention of weight regain are the long-term goals
What is Successful Weight Management? Natural Course of Weight Gain Starting weight Body weight (kg) Weight loss phase Weight maintenance Weight maintenance phase Months Years
3. Early intervention means addressing root causes and removing barriers • Successful obesity management requires identification and addressing of both the “root causes” of weight gain as well as the barriers to weight management • Emotional triggers and sleep deprivation are examples of root causes that can also pose significant barriers to weight management • Other causes of energy surfeit can include overeating, reduced physical activity or both
4. Success is different for every individual • Patients vary considerably in their readiness and capacity for weight management • Success can be defined as: quality of life improvements higher self-esteem or energy level improved overall health and sense of well-being modest (5%) weight loss prevention of further weight gain, or maintenance of the person’s best weight
5. A person’s best weight may never be an ideal weight • An “ideal” weight or BMI is not a realistic goal for most patients with obesity • Setting unachievable targets simply sets the patient up for failure • Set realistic and sustainable short-, intermediate, and long-term goals based on the “best” weight they can attain while still enjoying life and reaping the benefits of improved health
CPG Treatment algorithm for obesity Overweight or Obese Adult Measure BMI Measure WC (if BMI < 35 kg/m 2 ) Conduct clinical and Lab investigations to assess comorbidities BP, HR, fasting glucose & lipid profile Health team to advise lifestyle modification program Assess and screen for depression, eating and mood disorders Lifestyle modification program Treat comorbidities and/or health risks Nutrition: 500-1000 kcal/day reduction Physical Activity: Medical evaluation before starting activity. Assess barriers to weight loss and Initially 30 min of moderate activity 3-5 times/wk, eventually 60 min on most days. Add endurance readiness to change behaviours exercise training Cognitive-Behaviour therapy Devise goals and lifestyle modification program for weight loss & risk factor 5-10% of body weight loss or Satisfactory progress 0.5-1 kg (1-2 lb)/ week over 6 months or goal achieved Yes Regular monitoring No No Assist with weight maintenance Reinforce lifestyle modification Pharmacotherapy Bariatric surgery BMI 27 + risk factors BMI 35 + RF or BMI 40 Wt maintenance & prevent wt regain or BMI 30 Nutritional therapy Adjunct to lifestyle modification Consider if other weight loss attempts Physical Activity Consider if patient has not lost 0.5 kg or have failed. Cognitive-behavior therapy 1lb/wk by 6 months after lifestyle Requires lifelong medical monitoring Address other risk factors changes Periodic monitoring of body weight, BMI and WC every 1-2 years Lau DCW, et al. CMAJ 2007;176(8):1104-1106
Recommend










More recommend
Explore More Topics
Stay informed with curated content and fresh updates.