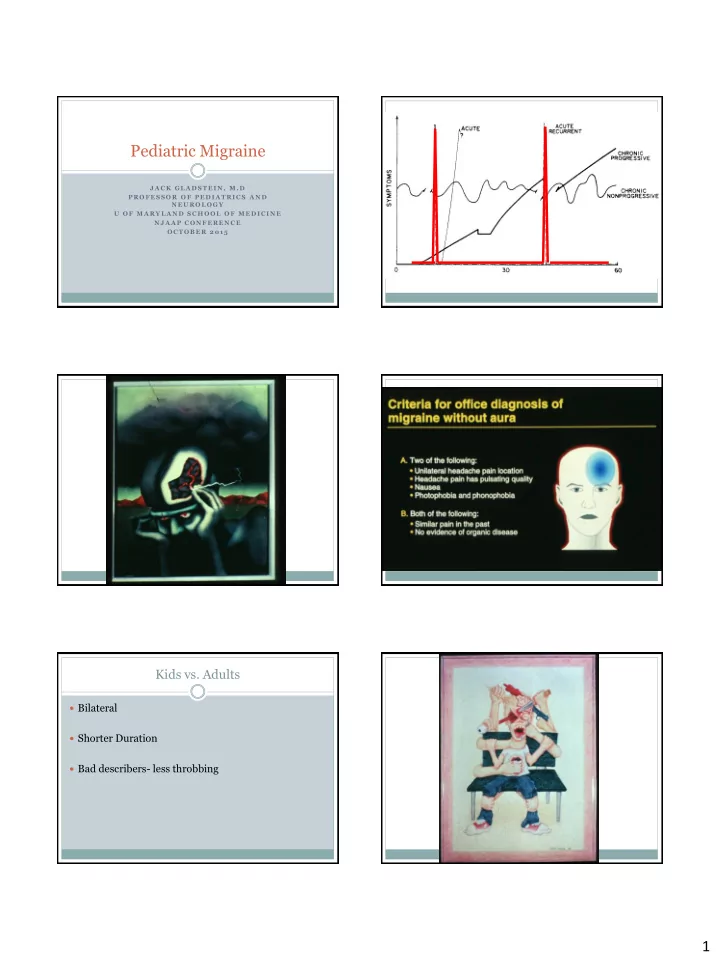
Pediatric Migraine JA C K GL A D ST EIN , M . D PR O FESSO R O F PED IA T R IC S A N D N EU R O L O GY U O F M A R Y L A N D SC H O O L O F M ED IC IN E N JA A P C O N FER EN C E O C T O B ER 201 5 Kids vs. Adults Bilateral Shorter Duration Bad describers- less throbbing 1
Do kids get allodynia? Migraine Summary Hershey Poster AHS: Acute and recurrent Severe As kids get older more allodynia Unilateral or Bilateral Girls > boys Usually No Aura Hair more than anywhere else Autonomic Symptoms Family history, relief with sleep Migraine Physiology Genetically Susceptible Trigger happens Decrease of Serotonin in MDR and Trigeminovascular system Open 5ht1-D receptor Physiology 2 MIGRAINE If autonomic symptoms : TENSION If not: 2
Sinus vs. Migraine SN(O)OP: Red Flags Pain over sinus can be due to firing of 2 nd branch of S ystemic Symptoms CN V N eurologic Symptoms O nset is abrupt So… N/V/ photo/Phono/ relief with sleep/ Pallor (O lder patient at onset for adults only) plus sinus tenderness : P revious Headache history is different MIGRAINE NOT SINUS For all Migraine Patients Weak Brain needs extra nurturing Sleep More and more regularly Eat Breakfast Drink Water Exercise Deal with Stress For All migraine patients STEP VS STRATIFIED CARE Treat attacks at first twinge Start Treat attacks with high doses of medication Don’t wait until sure it’s a migraine Involve school nurse and teacher A C A Start B B C 3
Acute Treatment Mixed drugs Analgesics: Aspirin, Acetaminophen, Ibuprofen, Midrin, Fioriset, Esgic Naproxen Sodium Gone out of favor Use higher doses! risk of medication overuse Adjunctive treatment 5-HT Agonists Antiemetics Route important Is there recurrence after dosing? anxiolytics Onset vs. duration Dihydroergoatamine Sumatriptan Can be given IV , IN, (or inhaled) Po, SQ, IN Multiple sizes give maximum flexibility Treximet- Imitrex 85 plus naproxen 500 4
Zolmatriptan Eletriptan PO, Melt and IN Po only 2 po doses, but 1 IN dose Almotriptan Naratriptan and Frovatriptan Pill only Slow in, long lasting May have a role in menstrual migraine prophylaxis May have role in bounce back headache Rescue Meds Match intensity to severity Have a role in Ed or Infusion Center setting IV MG More disabled- use triptans IV Fluids IV Steroids GET IT RIGHT FIRST TIME IV DHE IV Metochlopromide IV Valproate 5
Preventative strategies Initial Considerations Avoid Triggers Match intensity to severity Assess Coping skills More disabled- use triptans Assess Disability GET IT RIGHT FIRST TIME Absenteeism Presenteeism Prevention Drugs: Prevention Approaches Principles Cognitive Behavioral Therapy Who needs them? Biofeedback Absenteeism Presenteeism Relaxation Disability after retraining proper use of triptans Hypnosis Start low and go slow Acupuncture Realistic expectations Medications Prevention drugs: Which to choose? Amitriptyline Pick drug you are familiar with Start low: 10 mg . Increase weekly Pick drug that will give an extra bonus ? EKG Pick drug that will not exacerbate another problem Pick drug whose side effects will be tolerated by an INDIVIDUAL patient / family Weight gain, hard to wake up, dry mouth 6
Cyproheptadine Gabapentin Start low 4 mg Start low 900 mg Hard to wake up, weight gain Fuzzy sensorium, compliance a problem Pregabalin Topiramate Start low, but move fast Start slow 15-25 mg Brain fuzziness, weakness Weight loss, eye pain, dryness, subtle learning problems Propranolol Valproate Start slow 20 mg Start slow 500 mg Foggy, no exercise tolerance, depression, asthma Hair loss, fogginess exacerbation 7
Verapamil New treatments for next 5 years Start slow 40 mg Magnet ( next 2 years) Cefaly ( now) Sphenocath (now) Constipation , Orthostatic hypotension Inhaled DHE (asthma inhaler)(??) CGRP Monoclonal Antibody (5 years) (game changer) Magnet Cefaly Video <iframe width="560" height="315" src=https://www.youtube.com/embed/0Rh3btp7Rx w frameborder="0" allowfullscreen></iframe> Spenocath Inhaled DHE 8
CGRP monocloncal antibody Summary Diagnosis Easy Stratified Care Use Triptans Early and Often Get comfortable with a triptan and two prevention meds Refer when not sure 9
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries