NEW AND EMERGING TREATMENTS IN BULLOUS PEMPHIGOID NEIL KORMAN, MD, PHD PROFESSOR OF DERMATOLOGY UNIVERSITY HOSPITALS CASE MEDICAL CENTER CLEVELAND, OH
NEIL J KORMAN MD, PHD CONFLICTS OF INTEREST • Director of Clinical Trials Unit at UHCMC - many conflicts - none relevant to this talk • Consultant and Chair, Scientific Advisory Board - Immune Pharmaceuticals
BULLOUS PEMPHIGOID • Acquired subepidermal blistering disease • Most common autoimmune blistering dis • Primary lesion – tense blister on normal or erythematous skin • Often presents with urticarial plaques • Flexural arms, legs, abdomen, groin • Minority of pts have mucous memb disease
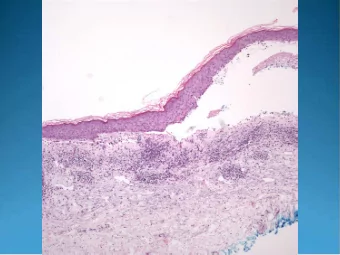
BULLOUS PEMPHIGOID HISTO/IMMUNOPATHOLOGY • Histopathology – Typically shows a subepidermal blister with an eosinophil rich inflammatory infiltrate • DIF – Almost all have linear BM C3 and most have linear BM IgG (some may have linear IgE) • IIF – Circulating IgG antibodies bind epidermal side of salt split skin
BULLOUS PEMPHIGOID ELISA • Tests for both BP 180 and BP 230 AB • Commercially available • ELISA Levels of BP 180 often correlate with disease activity
BULLOUS PEMPHIGOID COURSE AND PROGNOSIS • Typically lasts 1-5 years • Mortality rate vary depending upon pt country of origin • Generally less severe than pemphigus
BULLOUS PEMPHIGOID TREATMENT • Dictated by degree of involvement and rate of progression • Localized disease can be treated with topical steroids • RCT of topical vs oral steroids demonstrates both improved safety and efficacy of topicals over orals in moderate and severe dis • However in US majority of patients with generalized disease are treated with systemic steroids due to practical considerations • Many pts on oral steroids are given steroid sparing agents such as dapsone, doxycycline and niacinamide, MTX, MMF, AZA, Rituxumab and IVIg but quality of evidence supporting use of these medications is relatively low
CORTICOSTEROID TOXICITIES • Osteoporosis • Diabetes • HPA suppression • Glaucoma • Myopathy • Peptic ulcer • Osteonecrosis • Psychosis • Cataracts • Acne • Hypertension • Skin atrophy
PLANNED OR ONGOING TRIALS OF NON-BIOLOGICS IN BP • Two-arm, parallel group, 52-week RCT comparing the safety and efficacy of doxycycline (200 mg daily) with oral prednisolone (0.5 mg/kg daily) • Pts will receive fixed dose for the initial 6 weeks of treatment (doxycycline 200 mg daily; prednisolone 0.5 mg/kg daily), after which it will be adjusted as necessary. • 256 BP patients will be recruited in the UK and Germany. • A noninferiority analysis of doxycycline will be compared to prednisolone at 6 wks while safety will be assessed at 52 wks Br J Dermatol; 173:227-34, 2015 12
PLANNED OR ONGOING TRIALS OF NON- BIOLOGICS IN BP • RCT to compare efficacy and safety of topical clobetasol and methotrexate for 4 weeks followed by methotrexate alone for 8 months with topical clobetasol alone for 9 months • Primary endpoint will be 1 yr survival rate in both groups • Secondary endpoints will be the initial control rate of disease, the number of serious side effects during treatment and the number of relapses during treatment 13
EMERGING NEW BIOLOGIC TREATMENTS FOR BULLOUS PEMPHIGOID
OMALIZUMAB FOR TREATMENT OF BULLOUS PEMPHIGOID • 60 – 70% of BP pts have elevated serum IgE • 25% of pts have linear deposits of IgE at the epidermal BM on DIF • Omalizumab is a humanized monoclonal AB that blocks binding of IgE to its receptors • Omalizumab is FDA approved for treatment of asthma and chronic idiopathic urticaria
OMALIZUMAB FOR TREATMENT OF BULLOUS PEMPHIGOID • Open label study of 6 BP pts (urticarial plaques and bullae) • All had either elevated IgE or eosinophil counts • All had steroid refractory disease and were dosed at 300 – 400 mg q 2 – 6 wks • 5/6 pts responded to omalizumab • 3/6 pts responded to monotherapy • In 2/6 pts eosinophil counts correlated w/ disease activity • No significant toxicities were observed JAAD 2014;71:468-74
MORE BIOLOGICS WITH POTENTIAL IN BP AGENT MOA Bertilimumab: Anti Eotaxin-1 mAb Prevents Eotaxin-1-induced chemotaxis of eosinophils and neutralizes Eotaxin-1 in the circulation, preventing eosinophil migration Mepolizumab: Anti IL-5 mAb Prevents IL-5 mediated release of eosinophils from bone marrow into blood. Recently completed – no results yet Rituximab: Anti CD20 mAB Targets B cell by blocking CD20 on cell surface thereby preventing development of autoantibodies directed against BP antigens 17
MORE BIOLOGICS WITH POTENTIAL IN BP AGENT MOA IVIg Multiple different possible MOA’s QGE031: Anti IgE mAb Antibody directed against IgE. Clinical trial discontinued due to lack of efficacy TNT009 Anti-C1s antibody that selectively targets the classical complement pathway. Trial pending enrollment
EOTAXIN-1: A CHEMOKINE IMPORTANT IN EOSINOPHIL TRAFFICKING EOTAXIN-1-REGULATED • Mast Cells T cells CELL MIGRATION AND ACTIVATION Eosinophils Basophils EOTAXIN-1 Key Regulator in: Skin T cells CELLS SECRETING EOTAXIN-1 Macrophages Eosinophils 19
BERTILIMUMAB: MAB TARGETING EOTAXIN-1 • First fully human IgG4 mAb directed against eotaxin-1 • Safe, well tolerated in primates and in single administration to healthy volunteers: no SAE, no anti-drug antibody, high affinity and specificity for human eotaxin-1 • Selective, with rapid and lasting biological activity in Phase I 20
RATIONALE FOR TARGETING EOTAXIN-1 IN BP • Eotaxin-1 (Eo-1) is important for eosinophil transmigration • Eo-1 is incr in serum & skin lesions of BP patients • Eos co-localize w/basal keratinocytes w/incr Eo-1 & CCR3 expression • CCR3 is the main receptor on eosinophils • Eotaxin-1 is correlated with BP disease severity • Eotaxin-1 is expressed in Th2 cells in BP lesions Hence, Bertilimumab has the potential to eliminate the Eotaxin-1 positive feedback loop which is responsible for the recruitment of both eosinophils and Th2 cells to the site of inflammation in BP Br J Dermatol. 2007:454-9, Br J Dermatol. 2000 112-6, Acta Derm Venereol. 2000 277-80, Immunology and Cell Biology (2000) 78, 415–422; Respiratory Research 2001, 2:150-156, Clin Exp Immunol. 2002:470-8, Eur J Dermatol. 2002;12:27-31, Am J Reprod Immunol. 2004;51:32-9, Clin Exp Immunol. 21 2011;166:145-53, Am J Respir Cell Mol Biol. 1999:291-5 11. J Immunol. 1999;62:2946-55
EOTAXIN-1 LEVELS ARE INCREASED IN BP AND CORRELATE WITH DISEASE SEVERITY Levels of Eotaxin-1 are significantly Increased Eotaxin-1 up-regulated in serum of BP patients and both in sera and blister fluids correlates with disease severity* Eur J Derm, 12,27-31, 2002 Clin Exp Immunol. 2011;166:145-53 22
BERTILIMUMAB BP – PHASE 2 STUDY • Patients • Primary Objective To evaluate the safety of bertilimumab 10-15 adults newly diagnosed, moderate to extensive BP or pts on corticosteroids who • Secondary Objective cannot be successfully tapered To evaluate the preliminary evidence of clinical • Study design efficacy as measured by the BPDAI score (a severity Open-label, single group, 3 IV injections outcome measure), proportion of patients achieving (Day 0, 14, 28) of bert given along with 30 dose of prednisone 10mg/day at Day 84) mg/day oral prednisone, prednisone tapered down per protocol • Pharmacokinetics and Pharmacodynamics • Duration – Screening: up to 14 days • Exploratory Objective – Treatment period: 28 days (3 days) To determine change from baseline of biomarkers of – Follow-up period: 56 - 90 days (±3 days) inflammation Open to enrollment in Israel and the US – Total duration: 84 to 118 days (±3 days) 23 .
BERTILIMUMAB CASE STUDY SUBJECT 02-01 • 66 year old white male, newly diagnosed with BP • History of diabetes, diverticulosis, gastroduodenitis, anemia, hyperlipidemia • Concomitant medications: Lantus, sitagliptin, lansoprazole and iron supplement • Version 3 of the protocol, only 2 infusions bertilimumab given • Prior treatment: – 60 mg prednisone x 4 days, off 2 days, 40 mg 2 days, washed out for 2 weeks • BPDAI at Day 0 = 58; BPDAI at Day 60 = 3 • Patient’s last visit day 60 at 10 mg prednisone, tapered to 5 mg day 67
SUBJECT 02-01
SUBJECT 02-01
SUBJECT 02-01 – POST STUDY FOLLOW-UP – Treatment during the 2 following months: prednisone 5mg + 100mg minocycline – minor flares treated locally with clobetasol • Stop • No treatment for the next 4 months: – single periodic bulla treated with clobetasol – investigator defined pt as in remission
MEPOLIZUMAB (ANTI IL-5 AB) IN BULLOUS PEMPHIGOID • Investigator initiated randomized, placebo-controlled, phase 2, double-blind study of anti-IL-5 mAB in patients w/ BP. • Estimated Enrollment: 30 patients • Intervention: – Drug: Mepolizumab (an-IL-5 antibody) • 750mg mepolizumab four times over four months – Drug: Placebo • Saline placebo four times over four months • Study recently completed – results not yet available 28
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries