Maxim Transition Assist Maxim Transition Assist March 9 2016 March 9, 2016 1
Maxim Healthcare Services… Maxim Nationwide: Maxim Nationwide: 250+ offices across 40+ states • Approximately 60,000 caregivers and 46,000 patients nationwide • Specialized in skilled in ‐ home nursing care for the medically fragile and technology • dependent patient populations
The Maxim Transition Assist Approach The Maxim Transition Assist Approach Maxim Transition Assist Home Hospital • Transitional Care Nurse (RN) Home Assessment PCP Office PCP Office Final Transitional Care Plan • Community Health Worker (CNA) Pre ‐ hospital Care Post ‐ hospital Care Education and reinforcement Preliminary Risk Assessment (all Psychosocial support patients) Care Coordination Nurse Practitioner • • Program Manager Secondary Risk Assessment (high risk Scheduling patients) Staff coordination Preliminary TC Plan
The Readmission Problem… Approximately 20% of Medicare patients are readmitted within 30 days of • discharge (1) . The rate is higher for patients with certain conditions, such as COPD (20.9%), • congestive heart failure (24.7%) (approaching 50% at 6 months), HIV (26.4%), and co gest e ea t a u e ( . %) (app oac g 50% at 6 o t s), ( 6. %), a d chronic renal failure (27.4%). (2),(3),(4). In fact, for several conditions, such as sickle cell anemia, gangrene, hepatitis, and • white blood cell diseases, the 30 ‐ day readmission rate is over 30% (5). The transition from hospital to home is clearly a high risk period and drives a The transition from hospital to home is clearly a high risk period and drives a • substantial amount of medical spending. According to CMS, readmissions account for $26 billion in Medicare costs, of which $17 billion is potentially avoidable (6) . (1) Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee ‐ for ‐ service program. N Engl J Med. 2009;360(14):1418 ‐ 28. Epub 2009/04/03. doi: 10.1056/NEJMsa0803563. PubMed PMID: 19339721. (2) Ross JS, Chen J, Lin Z, Bueno H, Curtis JP, Keenan PS, et al. Recent national trends in readmission rates after heart failure hospitalization. Circulation Heart failure. 2010;3(1):97 ‐ 103. Epub ( ) , , , , , , f f p f ; ( ) p 2009/11/12. doi: 10.1161/CIRCHEARTFAILURE.109.885210. PubMed PMID: 19903931; PubMed Central PMCID: PMC2830811. (3) Butler J, Kalogeropoulos A. Worsening heart failure hospitalization epidemic we do not know how to prevent and we do not know how to treat! J Am Coll Cardiol. 2008;52(6):435 ‐ 7. Epub 2008/08/02. doi: 10.1016/j.jacc.2008.04.037. PubMed PMID: 18672163. (4) Elixhauser A, Steiner C. Readmissions to U.S. Hospitals by Diagnosis, 2010. HCUP Statistical Brief #153. April 2013. Agency for Healthcare Research and Quality (AHRQ). Epub 2013/04 . http://www.hcup ‐ us.ahrq.gov/reports/statbriefs/sb153.pdf. (5) Id. (6) CMS: Findings from Recent CMS Research on Medicare. Washington DC: Centers for Medicare & Medicaid Services, 2014. https://kaiserhealthnews.files.wordpress.com/2014/10/brennan.pdf. 5
The Real Problem… Psychological Factors Anxiety/Depression • Behavioral Disorders/ • Addiction Personality Disorders Readmission • Reduced Engagement Cognitive Impairment • Reduced Adherence Social Determinants Reduced Access Poor Housing/ • Homelessness Unemployment • Poor Education • Lack of Transportation • Readmissions are not the problem. Poor Nutrition • They are a symptom of larger underlying societal problems Lack of Caregiver • Support pp Dysfunctional Family • Dynamics Social Isolation •
The Readmission Solution… • Patient engagement at admission and continuity through post discharge period p g p • Transitional Care Team creates a partnership with the hospitalist, primary care and specialty care teams • Complements Home Health and other Post ‐ Acute Care Services • Focus on psychosocial barriers to adherence through Focus on psychosocial barriers to adherence through patient engagement and social service support
Role of the Community Health Worker Patient Engagement Frontline public health workers who are trusted members of the community served • Serving as a liaison between communities and health and social service systems • Health Education l h d Providing culturally appropriate health education • Care Coordination Ensuring people get community health services they need • Psychosocial and Medical Support Providing informal counseling and social support • Providing direct service, such as basic first aid and administering health screening • tests, when applicable tests, when applicable Community Empowerment Advocating for individual and community needs • Building individual and community capacity • Adapted from American Public Health Association Policy Statement 2001 ‐ 15 (Jan 2001).
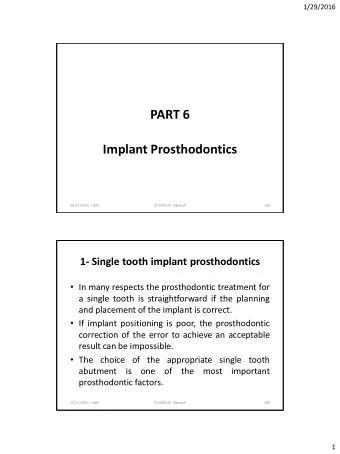
“High Risk” vs “Low Risk” Readmission Rates (h (hospital wide) it l id ) RightCare RA Rate (ADT Data) 18.0% 16.0% 14 0% 14.0% 12.0% 10.0% 8.0% 6.0% 4.0% 2.0% 0.0% Feb March April May June July August September RightCare High Risk Patients (RC Risk Score >= 3.0) 15.5% 12.7% 11.0% 9.2% 12.1% 15.5% 12.6% 8% RightCare Low Risk Patients 6.3% 4.7% 4.7% 6.8% 5.8% 7.0% 5.6% 4%
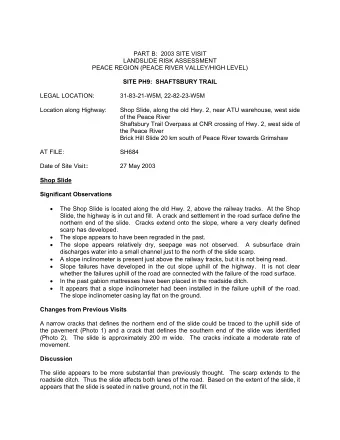
Readmission Rate for Program Participants vs non ‐ Program Participants P P ti i t MTA Program RA Rate (Program Data) Represents: 35.0% Discharged to LTC/SNF • 30.0% Discharged to SAR • 25 0% 25.0% Left w/o being seen • 20.0% Refused consent • 15.0% Other • 10.0% 5.0% 0.0% Feb Feb March March April April May May June June July July August August September September Consented/Admitted to MTA program (Completed 29.4% 23.3% 11.8% 16.7% 17.5% 18.5% 12.5% 13.1% NP Assessments) Not Admitted to MTA program (LWBS, SNF, SAR, 7.6% 7.8% 7.2% 4.1% 9.3% 11.1% 10.6% 6% Ref Consent, Other)
Take Aways… • 30 ‐ day hospital readmissions are a symptom of deeper underlying problems. • Maxim Transition Assist has reduced program participants’ 30 ‐ day readmission rates from 29.4% to 10.7%. • We’ve done this by creating a continuous partnership that We ve done this by creating a continuous partnership that engages patients and focuses on the underlying factors that increase risk of hospital readmission. • The core of our approach is the use of Community Health Workers. 11
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries