1. Biliary Drainage vs. No Biliary Drainage 2. Patency of Biliary Stents in Patients with malignant obstructive jaundice By James Monteiro de Barros, Niroshini Rajaretnam & S Aroori
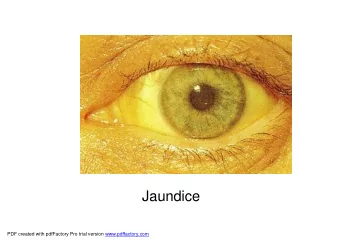
Biliary Drainage • Obstructive jaundice is common • Malignant and benign causes • Before 1980s- surgery is the treatment of choice • Jaundice can lead to – Hepatic dysfunction – Cholangitis – Cirrhosis – Severe pruritus – Weight loss
Benefits of Biliary Drainage • Less yellow • Itching goes away • Patients feels better • Taste/eating improves
Types of Biliary Stents • Plastic • Metal – Covered – Uncovered • Length • Diameter
Metal stents • Resectable tumours – we would prefer short covered metal stent • Life expectancy < 4 months – Plastic stent • Life expectancy > 4 months – Metal stent
Types of Biliary Drainage • Endoscopic drainage (EBD) – External – Internal • Percutaneous drainage (PTBD) – External (Nasal) – External (Skin)
EBD • Bleeding • Pancreatitis • Blocked stent • Cholangitis • Size of the stent- standard duodenoscope 4.2mm diameter • No loss of electrolyte abnormalities
PTBD Disadvantages • Dislodgement • Collapse of the stent • Discomfort • Blockage • Cholangitis • Electrolyte abnormalities • No sphincterotomy
Key Questions • 1) How does routine pre-op drainage vs non pre-op drainage compare in terms of mortality and morbidity? • 2) How does pre-op biliary drainage through endoscopic and percutaneous approach compare in terms of efficacy, complications, survival, quality of life and cost? • 3)Hoes does plastic and metal stents compare for pre-op drainage in terms of re-intervention, survivability, mortality and cost?
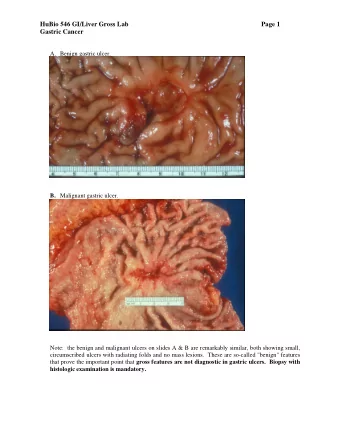
Evidence • ESG October 2017 Against routine pre-op biliary drainage Not recommended for malignant biliary obstruction who need surgery. Exceptions Cholangitis, delayed surgery, neo-adjuvant and intense pruritus. Bilirubin > 250. 10 Meta-analyses found no difference in mortality, but increased morbidity if they have had drains.
Evidence • If drainage is indicated – Self expanding metal stents were associated with lower rates of re- intervention. 3.4% vs 14.8% (plastic). – No difference in mortality and morbidity between the stents. – Fully covered metal stents show longer patency compared to uncovered metal and plastic stents in patients undergoing neo- adjuvant chemotherapy – Presence of stents does not affect resectability but prolongs the duration of surgery. – External drainage vs internal drainage has decreased survival
Scope • Study looking at patients referred to Plymouth HPB MDT with presumed – Head of Pancreas Cancer – Ampullary Cancer Requiring a – Duodenal Cancer biliary stent – Distal cholangiocarcinomas – Hilar cholangiocarcinomas • Retrospective study – 2011 to 2014 inclusive
Hypotheses, Aims and Objectives • Hypothesis A – Are patients with curative intent having delayed operations due to complications arising from their stents • Hypothesis B – Patients with curative intent require stents as surgery cannot be achieved in the required time
Jan 2011-Aug 2012 • 215 referrals to the HPB MDT Hospital Number of HoP & Amp Ca Cholangio Patients Duodenal Ca Barnstaple 17 12 2 3 Exeter 29 17 6 6 Plymouth 100 66 8 26 Torbay 33 17 5 11 Truro 36 29 1 6
Plymouth • 50 female and 50 male • Age at referral 64 71 78 91 35 • Presentation
Initial Outcomes 100 patients • 2 – no stent/palliated • 3 – theatres without stent • 40- stented theatre after stent • 55 – palliative stent
Theatre Cohort • 40 with curative intent (stented group) – 25 had a Whipple’s procedure – 4 Extra hepatic bile duct reconstructions – 2 liver resections and bile duct reconstructions – 8 bypass operations for locally advanced cancer or metastases – 1 open and close case
Theatre Cohort Wait after stent 39 patients 4-8 weeks Neoadjuvant <2 weeks 2-4 weeks >8 weeks chemo 6 patients 1 patients 2 patients 21 patients 10 patients 2 Whipple’s 3 Whipple’s 13 Whipple’s 7 Whipple’s 1 Whipple’s 1 bypass 5 bypass 1 bypass 1 liver 1 liver 1 liver 1 Roux 1 Roux 1 Roux 1 open & close
Were stent complications a cause for delayed operations? • 9 /40 (22.5%) re-admissions • 7/40 (17.5%) re-admissions due to Blocked stents/stent complication • 2-4 weeks post stent placement – 1 stent complication requiring admission. Bypass as mets found • 4-8 weeks – 6 stent complications requiring admission. All of them plastic stents (with complications 4-21 days after initial ERCP/PTC). All of them went onto a Whipple’s • >8 weeks – 2 stent complications during prolonged initial admission due to pancreatitis/AKI. Both went onto a Whipple’s
Palliative Stents • 3/55 (5%) died within 7 days of insertion • 29/55 (53%) patients did not have any admissions due to stent blockages/stent complications – 4 plastic (18-88 days) – 25 metal (13-612 days) median 273 days • 5/55 (9%) patients required an exchange of stent
Blocked Palliative Stents • 17/55 (31%) had at least one blockage/stent complication • 10 Plastic (8-459 days) median 56 days – 9 having a metal replacement stent & 1 palliated • 9 Metal (66-1454 days) median 274 days – 7 having a metal replacement stent & 2 palliated
Survival • 1 patient with a P2N0R0 ampullary cancer is still alive > 6 years with no recurrence • 4 patients who underwent a Whipple’s or bile duct reconstruction are still alive - histology gallstones or chronic pancreatitis. • Curative intent – 33-2136 days, median 682 • Palliative cohort – 5-1995 days, median 149 – Outlier at 1995 days with presumed low CBD cholangiocarcinoma. No treatment as too co-morbid
Conclusion • Study is still ongoing • Tentative conclusion – Whilst stents do cause admissions at 17.5% – More data is required to demonstrate if it causes major delays in patients having surgery.
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries