
SLIDE 1
5/26/2018 1
Impact of WHO 2017 and AJCC 8th edition
- n Gastropancreatic
Neuroendocrine Neoplasms
Grace E. Kim, MD
Disclosures
Shareholder
- Five Prime Therapeutics and Adicet Bio
Consultant
- Celgene
These companies and its products will not be discussed in this presentation
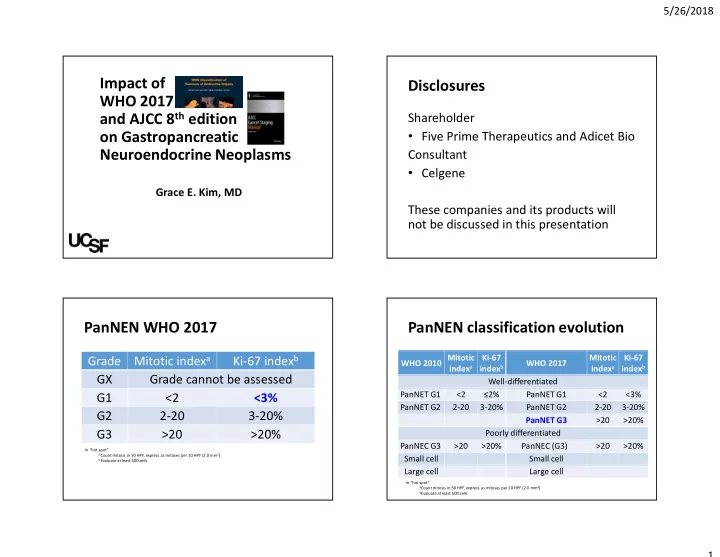
PanNEN WHO 2017
Grade Mitotic indexa Ki-67 indexb GX Grade cannot be assessed G1 <2 <3% G2 2-20 3-20% G3 >20 >20%
In “hot spot”
a Count mitosis in 50 HPF, express as mitoses per 10 HPF (2.0 mm2) b Evaluate at least 500 cells
PanNEN classification evolution
WHO 2010 Mitotic indexa Ki-67 indexb WHO 2017 Mitotic indexa Ki-67 indexb Well-differentiated PanNET G1 <2 ≤2% PanNET G1 <2 <3% PanNET G2 2-20 3-20% PanNET G2 2-20 3-20% PanNET G3 >20 >20% Poorly differentiated PanNEC G3 >20 >20% PanNEC (G3) >20 >20% Small cell Small cell Large cell Large cell
In “hot spot”
aCount mitosis in 50 HPF, express as mitoses per 10 HPF (2.0 mm2) bEvaluate at least 500 cells