
How do I tell if its benign PVCs or ARVC? Robert M. Hamilton The - PowerPoint PPT Presentation
How do I tell if its benign PVCs or ARVC? Robert M. Hamilton The Hospital for Sick Children & Research Institute Autopsy from Ten Year Old Female following Sudden Cardiac Death Why differentiate RVOT VT/PVCs from A(RV)C? }
How do I tell if it’s benign PVC’s or ARVC? Robert M. Hamilton The Hospital for Sick Children & Research Institute
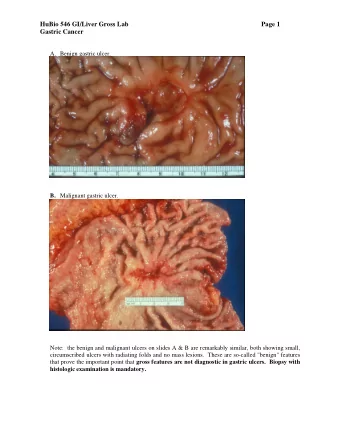
Autopsy from Ten Year Old Female following Sudden Cardiac Death
Why differentiate RVOT VT/PVC’s from A(RV)C? } 25% RVOT VT is relatively benign ARVC is a progressive disease and a significant cause of sudden cardiac death. Even in Children! Tabib, 2003 DuPuis, 2005 Pilmer, 2014
Right Ventricular Outflow Tract VT(PVC’s) Monomorphic VT originating from RVOT Usually no underlying structural heart disease May also occur in the context of ARVC Heart rate > 100 bpm. QRS duration > 120 ms. LBBB Morphology Rightward / inferior axis (around +90 degree) ± VA dissociation.
Right Ventricular Outflow Tract VT Two predominant forms (Lerman et al, 1996) repetitive monomorphic nonsustaincd VT paroxysmal exercise induced sustained VT
48 Children with RVOT VT (5 Centers) 8.2 yrs (0.1-17.0 yrs); F/U 22 mo. (1-210 mo.) 82% referred for incidental finding, but 46% reported symptoms to cardiologist 15% referred for syncope or near-syncope 40% had a history of exercise intolerance 10% had a family history of arrhythmia
MRI performed in 25 (52%) abnormalities in 13 (wall thinning in 8, fatty infiltration in 4, fibrosis in 2, and dyskinesia in 2) Biopsies performed in 12 (25%) Minor changes in 5 (fibrosis, interstitial lymphocyte infiltration, interstitial edema, and mild hypertrophy) Catheterization performed in 11 (23%) findings included focal dyskinesia in 1, apical hypokinesia in 1 & segmental wall-motion abn. in 1 Some may have had early ARVC, but no deaths occurred
Derivation Cohort: 16 ARVD/C v. 42 RVOT-VT Validation Cohort: 37 ARVD/C v. 49 RVOT-VT ARVD/C met task force criteria RVOT-VT Structurally Nl, Successfully Ablated
No difference in Sx or Exercise-related Sx FH in 60% of ARVC, 0% of RVOTO-VT Abn ECG in 52% of ARVC. T-inv. In 36% Abn SAECG in 78% of ARVC, NoRVOTO-VT All RVOT-VT and 53% of ARVC: inf. axis VT 42% of ARVC had 2+ morphologies of VT PES ind. VT in ARVC, Isuprel in RVOT-VT Fragmented Potentials v. Presystolic Potentials
Compared LBBB-Inf. Axis Arrhythmias between ARVC and RVOT-VT Follow-up not stated ARVC had: Longer mean QRSdd (150 ± 31 v. 123 ± 34 ms) Precordial transition in V6 (3/17 v. 0//42) Notching in 1+ lead (11/17 v. 9/42)
Differentiating RVOT VT from ARVC Feature RVOT VT ARVC Mechanism Unifocal LBBB Nl Axis Re-entry (slow conduction) PVC’s Unifocal LBBB Nl Axis Multifocal LBBB VT Repetitive MMVT+/or Stress-related MMVT Paroxysmal Ex.-ind. QRS Normal +/- prolonged S duration in V1 Normal +/- prolonged SAECG Normal +/- prolonged MRI Normal +/- RV dil & dysk T-wave altenans Negative +/- positive Ablation Success in 94% Var. success and recurrence Family History VT/SCD Negative Often Positive Genetic basis Somatic mutation in Desmosomal in 1/3
General observations Understanding PVC’s is complex. They are capricious. Often can’t find out why they come, leave, come back. Response to exercise helpful but not absolute (Gross) PVC’s are defined by the company they keep (Usially benign if isolated and heart is structurally and functionally normal) Freq. PVC’s or isolated RVOT VT = a single minor Task Force criterion (ARVC unlikely)
My Approach Take a family history! Asymptomatic PVC’s Assess morphology: RVOT vs. LV vs. RV body ECG, Holter , SAECG (≥5), Ex. Test (≥6), Echo Consider 12-lead Holter, ? T-wave alternans Not RVOT morphology, multiple morphologies or abn SAECG or Echo: MRI (≥9) Minimally symptomatic (palpitations) Non-invasive monitors Symptomatic (syncope: non-vasodepressor) MRI, genetics, ± EP study, ILR ?ARVC: Genetics, biomarker in development
Master Thesis Sarah Vermij Q (Toon van Veen) U June 2014 E S T I O N S ? robert.hamilton@sickkids.ca
Recommend











More recommend
Explore More Topics
Stay informed with curated content and fresh updates.