High clinical utility the potential for fewer risky procedures and - PowerPoint PPT Presentation
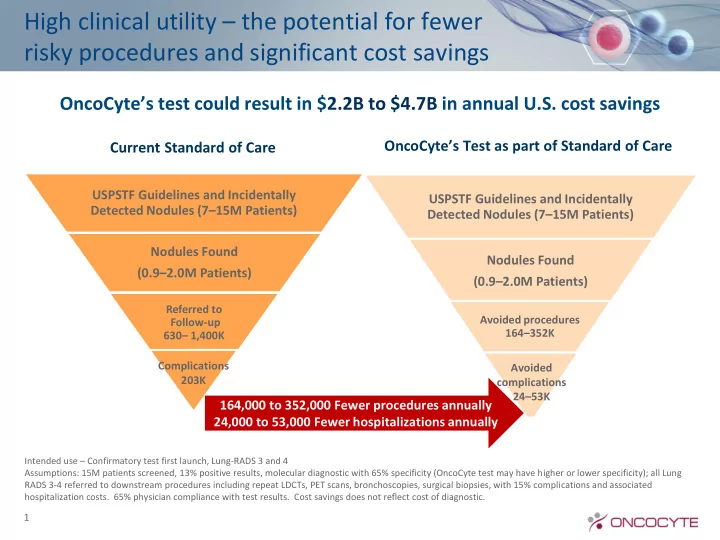
High clinical utility the potential for fewer risky procedures and significant cost savings OncoCytes test could result in $ 2.2B to $4.7B in annual U.S. cost savings OncoCytes Test as part of Standard of Care Current Standard of Care
High clinical utility – the potential for fewer risky procedures and significant cost savings OncoCyte’s test could result in $ 2.2B to $4.7B in annual U.S. cost savings OncoCyte’s Test as part of Standard of Care Current Standard of Care USPSTF Guidelines and Incidentally USPSTF Guidelines and Incidentally Detected Nodules (7 – 15M Patients) Detected Nodules (7 – 15M Patients) Nodules Found Nodules Found (0.9 – 2.0M Patients) (0.9 – 2.0M Patients) Referred to Avoided procedures Follow-up 164 – 352K 630 – 1,400K Complications Avoided 203K complications 24 – 53K 164,000 to 352,000 Fewer procedures annually 24,000 to 53,000 Fewer hospitalizations annually Intended use – Confirmatory test first launch, Lung-RADS 3 and 4 Assumptions: 15M patients screened, 13% positive results, molecular diagnostic with 65% specificity (OncoCyte test may have higher or lower specificity); all Lung RADS 3-4 referred to downstream procedures including repeat LDCTs, PET scans, bronchoscopies, surgical biopsies, with 15% complications and associated hospitalization costs. 65% physician compliance with test results. Cost savings does not reflect cost of diagnostic. 1
Physicians in target specialties express highest level of interest Interest in Using OncoCyte Product 9.3 10 8.7 8.5 8.3 9 7.8 8 7 6 5 4 3 2 1 Total Oncologists Radiologists Interventional Pulmonologists radiologists • Interest in using the OncoCyte test is very high (mean rating of 8.5 out of 10) • Highest interest with pulmonologists and interventional radiologists • Reasons provided for high ratings: Useful for smaller nodules with high risk factors Provides additional accuracy and benefit Avoid biopsies Non-invasive blood test Provides clinical utility Results of (30) in-depth, clinician interviews fielded in September/October 2015. Question asks: 2 On a scale from 1-10 where 10 is very interested, how interested would you be in utilizing Test X?
Reimbursement strategy has three key components • MAAA Ensured status allows value based pricing • Pursue CDLT status • Launch with unlisted code Coding • Obtain unique CPT code when have CMS coverage • MolDx has clear pathway to coverage • Develop and implement a strong evidence and publication plan • Clearly demonstrate analytical and clinical validation, clinical utility and cost savings to health care system Coverage • Obtain CMS coverage 2-3 years after launch • List price at launch • CMS Price set post-launch based on weighted average of commercial plans Reimbursement • Pursue private payor strategy that leverages PAMA pricing guidelines • Optimize rather than maximize in-network providers 3
Lung is compelling proposition for payers “Getting tissue in lung biopsy is much more invasive for lung than other cancers” “Am concerned with USPSTF guidelines and the high false positives (one in five) and invasiveness of biopsies” “Not just about the expense, there is also increase morbidity and mortality with biopsies” “High need driven by lack of good screening procedures and • Payers gave diagnostic high ratings for unmet needs a clinical concern to identify • Pricing and TPP discussion with payers very positive patients earlier” Survey of (10) Commercial, Managed Medicaid and Managed Medicare payers representing 20M covered lives. Question asks: What is your perception of the overall unmet need for certain oncology screening diagnostics or procedures. 4 On a scale of 1 to 10 where 1 is no unmet need and 10 is significant unmet need for an improved screening procedure/diagnostic.
Key to coverage is strong clinical validation and clinical utility studies MolDx Coverage Pathway MolDx Clinical Trial Clinical Trial • OncoCyte’s strategy is to achieve Level of Design Principal Design Evidence Study Secondary the highest level (IA) of evidence Study Highest IA Randomized, Randomized • Prospective (PCT) Prospective or Previewed clinical protocol designs Retrospective with payers (November 2016) (PCT, PRT) Coverage Probability – 10 Payers IB PCT` Prospective Observational – Public and commercial Studies (POS) or Retrospective – 77M Covered lives Data Modeling (RDM) IIA PRT POS or RDM IIB POS POS or RDM (minimum requirement) Conclusion: Successful trials should result in positive coverage decisions. 5
Focused reimbursement strategy enables value-based pricing PAMA Ensures Optimize Value-based maintenance of private-payer pricing creates value-based coverage list price pricing • Contracting strategy • OncoCyte test is MAAA • Medicare price determined focused on maintaining every 12 – 36 months based • Full list price for the value-based pricing on weighted commercial first six months of • Patient assistance median Medicare coverage program 6
Recommend





More recommend
Explore More Topics
Stay informed with curated content and fresh updates.